
CR3-193
The novel use of high-dose hydroxycobalamin for vasoplegic syndrome in a pediatric patient after cardiopulmonary bypass.
Patel P, Scott J, Loveland-Baptist L, Hoffman G, Voulgarelis S
Children's Hospital of Wisconsin, Milwaukee, WI, USA
Introduction
We describe a case vasoplegic syndrome (VS) after cardiopulmonary bypass (CPB) treated with hydroxocobalamin (B12) in a child with failed Bidirectional Glenn (BDG) physiology. To our knowledge, this is the first documented use of B12 for pediatric CPB related VS.
Case Report
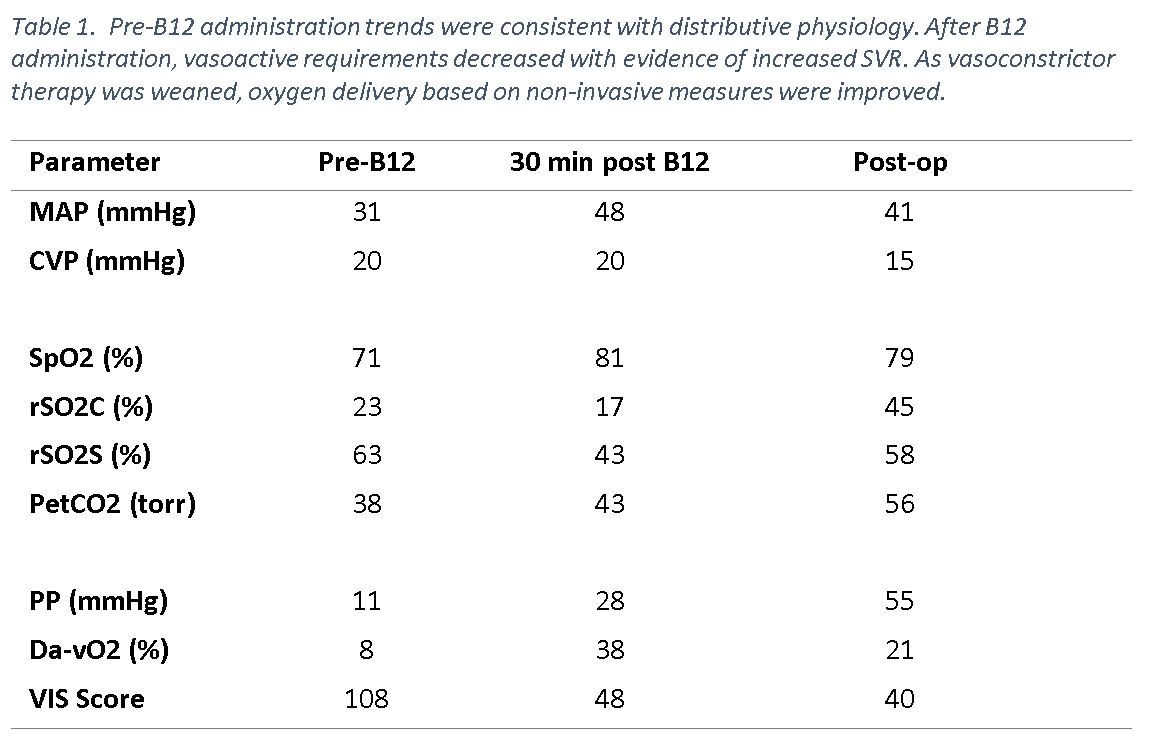
Six m/o male with HLHS s/p BDG who exhibited severe hypoxia with elevated transpulmonary gradient coincident with a large thrombus extending from the left internal jugular vein to the innominate vein. The patient underwent thrombectomy on CPB, and required VA ECMO for persistently elevated BDG pressures, hypoxia, and cardiogenic shock. He continued to require significant vasoactive support while on ECMO and developed multiorgan system failure. After partial recovery, he underwent modified 3.5 mm BT shunt and ECMO decannulation. After weaning from CPB there was minimal vasoconstrictor response to norepinephrine, vasopressin and hydrocortisone. Vasoplegia persisted until B12 was administered; 70mg/kg IV X 3. Hemodynamics improved, and vasoconstrictor requirement was significantly reduced. The patient remained off of ECMO. However, he eventually developed oliguric renal failure, hyperkalemia, and persistent multiorgan failure. Support was later withdrawn.
Discussion
Vasoplegic syndrome has an incidence ranging between 5% and 15%.[1] Risk factors include ACE inhibition, beta blockade, and long CPB times. [1] Hypotension at the onset of CPB is another risk factor. [1] The etiology of VS is multifactorial, but is thought to be due to abnormal activation of inflammation and vasodilation. Specifically, VS is thought to be related to a dysfunction of nitric oxide mediated vascular smooth muscle resistance. [2] Treatment of VS includes alpha-agonists, vasopressin, and nitric oxide scavengers like methylene blue. Methylene blue is associated with adverse effects such as hemolytic anemia, serotonin syndrome, methemoglobinemia, and pulse oximetry interference. [2]
Vitamin B12 is approved for cyanide poisoning (70mg/kg IV, may repeat based on clinical response) forming a nontoxic cyanocobalamin, which is then excreted. [3] The mechanism by which B12 is efficacious in treating VS is unclear. Studies suggest nitric oxide and carbon monoxide scavenging as a possible mechanism for B12 mediated reversal of VS. [4] Side effects of B12 include hypertension and increased systemic vascular resistance (SVR) as well as rash, erythema, dysphagia and chromaturia. [3] Our patient experienced rash, chromaturia, and increased SVR. This case highlights B12 use to treat VS after pediatric CPB. However, it is unclear whether the side effect profile makes B12 a safe treatment strategy for vasoplegia after CPB in children.
Sources
1. Levin MA et al. Circulation 2009; 120:1664–71.
2. Roderique JD, et al. Ann Thorac Surg 2014;97: 1785–6.
3. Burnes ML, et al. J Cardiothorac Vasc Anesth 2017; 31:1012-1014
4. Gerth K, et al. Clin Toxicol (Phila) 2006; 44(Suppl 1):29–36.
-
 CR3-193 Image 1
CR3-193 Image 1
Top










