
GA2-59
Anesthesia for Pediatric Patients with Anti-NMDA-Receptor Encephalitis: a retrospective case series.
Friedman M, Bell M, Matar M, Ross P, Nagoshi M
Children's Hospital Los Angeles, Los Angeles, CA, USA
INTRODUCTION
Anti-N-Methyl-d-Aspartate receptor (NMDAR) encephalitis is a neurologic condition caused by auto-antibodies that target the NMDAR. Since the first pediatric case report in 2007, it has become the second most common cause of autoimmune encephalitis in children.
Patients present with psychosis, neurologic deficits, seizures, with progressive decline to decreased responsiveness, catatonia, and paroxysmal sympathetic hyperactivity. Most recover completely, but a small percentage are left disabled or die from an arrhythmia.
The NMDAR is commonly targeted by anesthetic agents. Other than ketamine, nitrous oxide, and methadone, the NMDAR may be associated with the action of volatiles, propofol and midazolam. Therefore, these patients may have unique anesthetic interactions.
There are few case reports of pediatric patients with anti-NMDAR encephalitis receiving anesthesia, and no case series. These patients almost always require anesthesia during diagnostic workup. We hypothesize that these patients are potentially vulnerable to hemodynamic (HD) instability under anesthesia.
METHODS
We performed a retrospective chart review of 30 anesthetics in 19 patients. Our primary outcome was the presence of HD instability and arrhythmias under anesthesia or post-anesthesia.
Primary analytic endpoints include: heart rate (HR), systolic and diastolic blood pressures (SBP & DBP), respiratory rate (RR), oxygen saturation (SAT), and temperature (TEMP) pre-anesthesia, post-anesthesia, and at 15, 30, 45, and 60 minutes during anesthesia.
A generalized estimating equation regression model with log scale approach was used to examine the percent change in these endpoints compared to baseline.
RESULTS
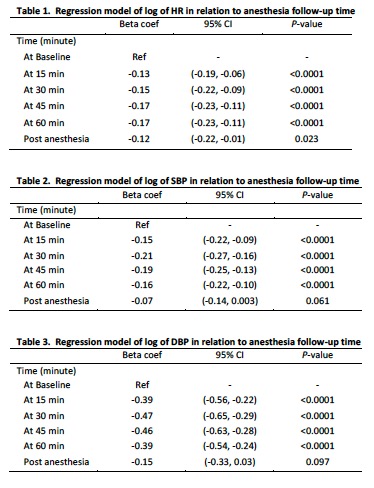
As noted in tables 1-3, there was a statistically significant decrease in HR, SBP, and DBP from baseline at 15, 30, 45, 60 minutes.
There were no statistically significant changes in RR, SAT, or TEMP from baseline, nor arrhythmias reported under anesthesia.
One child suffered an arrhythmia leading to sudden death within 24 hours of anesthesia. Another had extreme hypertension and tachycardia in PACU.
DISCUSSION
We can conclude that these patients experienced a statistically significant change in HR, SBP and DBP at 15, 30, 45, 60 minutes. However, these changes were not clinically significant enough to warrant intervention, even in the child who died.
This supports our hypothesis these patients may be more prone to HD instability while under anesthesia. Although the clinical significance is yet to be determined, this is important in a population with increased risk of sudden cardiac death.
In the case of sudden death, that patient presented late in the disease process, and was having more severe symptoms. Perhaps this is a risk factor for peri-operative complications.
CONCLUSION
Anesthesia providers must be aware of the potential for HD instability, arrhythmias, and sudden cardiac death in this patient population.
-
 GA2-59 Image 1
GA2-59 Image 1
Top










