
NM-361
Changes in cerebral oxygenation during laparoscopic pyloromyotomy
1Hakim M, 1Walia H, 2Kamada M, 3Miller R, 4Tumin D, 1Tobias J
1Nationwide Childrens Hospital, Columbus, Ohio, USA; 2Saitama Childrens Medical Centre, Hidaka, Yamane, Japan; 3Nationwide Childrens Hopsital, Columbus, Ohio, USA; 4Natinowide Childrens Hospital, Columbus, Ohio, USA
Background: Maintaining cardiac output and oxygen perfusion to the tissues is important during intraoperative care. While monitoring vital parameters such as blood pressure and heart rate are routine, there is interest in measuring cerebral and end organ tissue oxygenation in various clinical scenarios. We analyzed cerebral and tissue oxygenation using near infrared spectroscopy (NIRS) in infants undergoing laparoscopic pyloromyotomy using cerebral and flank oximetry (rSo2). The primary outcome of our study was to evaluate changes in cerebral and tissue oxygenation during abdominal insufflation for laparoscopy.
Methods: Following IRB approval, infants ≤ 3 months of age undergoing laparoscopic pyloromyotomy were recruited for the study. Cerebral and tissue oxygenation were measured using NIRS. Average cerebral and tissue oxygenation levels were calculated prior to induction, after induction, at incision, at the beginning of laparoscopy, at the end of laparoscopy, and at the end of surgery. Oxygenation levels at incision and at the end of laparoscopy were compared using a paired t-test.
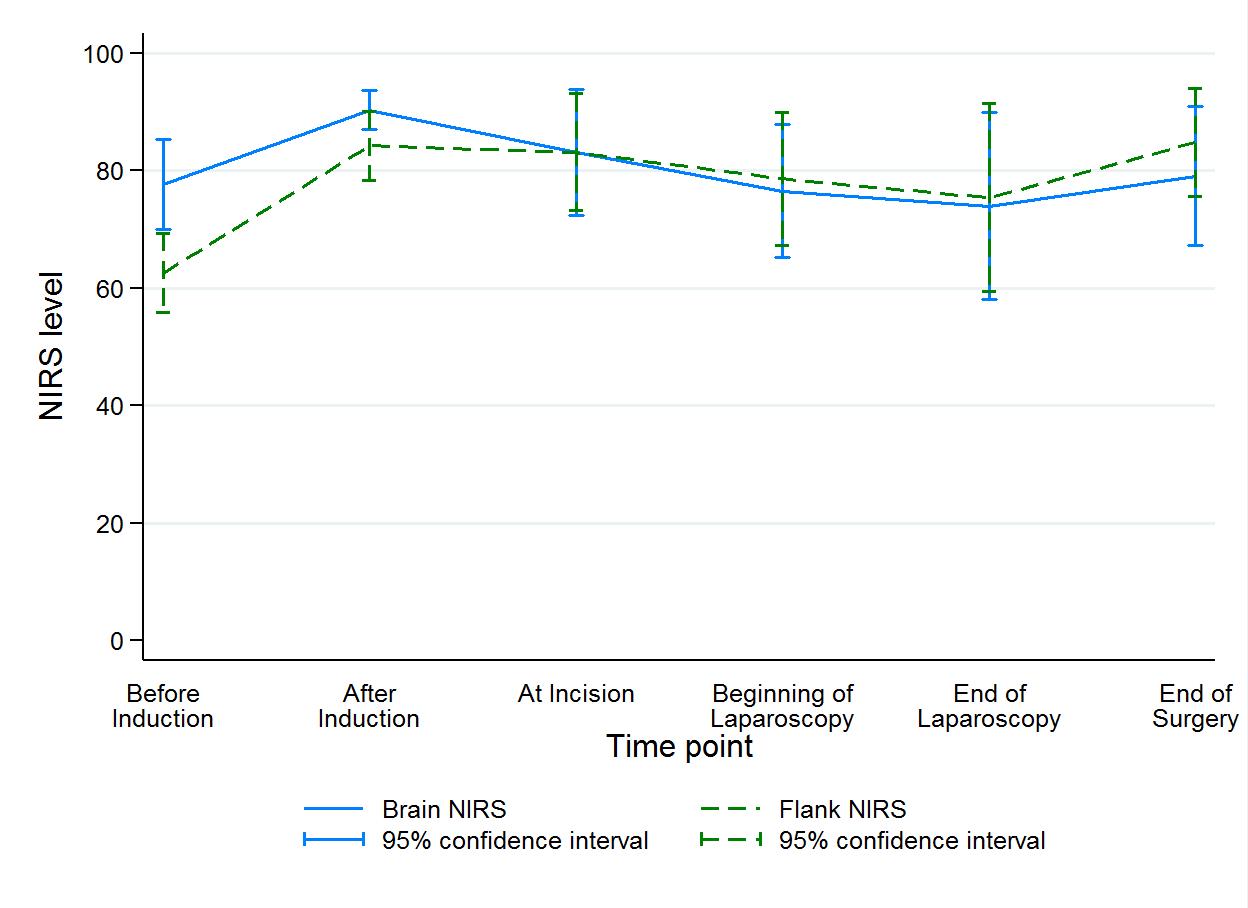
Results: The study cohort included 11 patients (6 male and 5 female) with an ASA status of I-III. Mean intra-abdominal pressure at the beginning of laparoscopy was 10 ± 3 mmHg. Changes in NIRS over the course of the procedure are shown in the Figure. Cerebral rSO2 before induction was 78 ± 10 and tissue rSO2 was 63 ± 9. After anesthetic induction, cerebral rSO2 was 90 ± 5 and declined significantly to 74 ± 24 after laparoscopy (CI difference: 1, 32; P=0.040). Tissue rSO2 showed a non-significant decline from 84 ± 9 after induction to 75 ± 22 after laparoscopy (CI difference -7, 25; P=0.247).
Discussion: Cerebral oxygenation decreased significantly between anesthetic induction and the end of laparoscopy. However, the nadir cerebral oxygenation was only 1% below the value noted in the awake state prior to anesthetic induction. No change in tissue oxygenation was noted. Insufflation of the peritoneum and the increase in intra-abdominal pressure (IAP) may increase systemic and pulmonary vascular resistance thereby decreasing cardiac output and ultimately tissue oxygenation in infants during laparoscopic procedures. Other factors including hypercarbia and Trendelenburg position may also impact cerebral oxygenation.
Conclusion: Cerebral oxygenation declined significantly during laparoscopic pyloromyotomy
-
 NM-361 Image 1
NM-361 Image 1
Top










