
GA2-63
Embolization and Tranexamic Acid to Reduce Bleeding in Resection of Intracranial Juvenile Nasopharyngeal Angiofibroma
Houska N, Hammon D, Downard M
Wake Forest School of Medicine, Winston Salem, North caro, United states
Learning Objectives
1. Formulate a multimodal approach to reduce blood loss in high grade (intracranial) JNA.
2. Demonstrate that tranexamic acid (TXA) can be utilized to reduce blood loss and transfusion volume in JNA resection
Preoperative Course
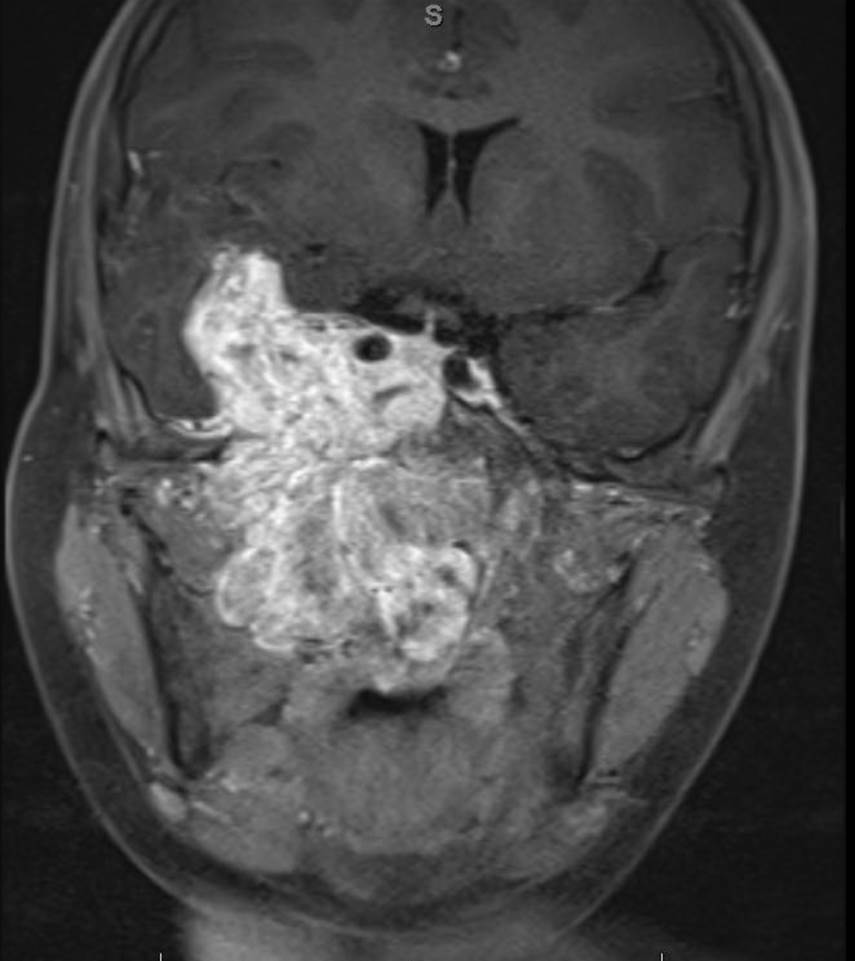
A 9-year-old, 43 kg, male with no past medical history for resection of a large JNA with intracranial extension. MRI showed a large mass (9.2 × 5.2 × 5 cm ) with compression nasopharynx and elevation of the temporal lobe. He failed a course of chemotherapy and was referred for resection with prior embolization. The day prior to surgery he underwent successful embolization of the arterial blood supply from the external carotid, while the internal carotid feeders could not be occluded.
Case Description
On day of surgery the patient had: a radial arterial line, two 18 g PIVs, hemoglobin10.5 g/dL, crossmatched blood. Uneventful induction and intubation. Anesthesia was maintained with volatile and opioid infusion. The following techniques were utilized to reduce blood loss: hypotension with a MAP goal of 55-60, reverse Trendelenburg position, TXA bolus of 20 mg/kg followed by 10 mg/kg/h infusion intraoperatively. Cell salvage was avoided at surgeon request. The intracranial tumor was resected followed by the nasopharyngeal burden. Ins and outs: blood loss 950 mL; fluids 3900 mL crystalloid, 885 mL pRBCs, 600 mL plasma. The patient had no significant hemodynamic instability and extubated at the end of his 10.5 h procedure. Postoperative hemoglobin 9.8, pH normal, base deficit 2.8.
Discussion
The potential for catastrophic blood loss is one of the most challenging aspects of JNA resection and is associated with increased morbidity and mortality. Numerous techniques have been utilized to reduce blood loss including: reverse Trendelenburg position, induced hypotension, cell salvage, and preoperative embolization. Embolization is utilized by most centers and has been shown to reduce quantity transfused blood in high grade tumor resection, but not necessarily improve outcomes.Tranexamic acid, an antifibrinolytic has been widely utilized to reduce blood loss and transfusion in pediatric cardiac, orthopedic, trauma, and craniofacial surgeries.1 Literature review showed anecdotal use of antifibrinolytics for resection, and one study comparing the use of aminocaproic acid versus TXA in low grade NPA resection.2 Given that high grade tumors with intracranial extension tend to have more blood loss and increased morbidity, there appears to be a dearth of knowledge in the use of TXA to reduce blood loss. While we had good outcomes with our use of TXA in combination with embolization, further research needs to be conducted to determine if the benefits outweigh the risks.
References
1. Goobie SM, Meier PM, Pereira LM, McGowan FX, Prescilla RP, Scharp LA, Rogers GF, Proctor MR, Meara JG, Soriano SG, Zurakowski D, Sethna NF. Efficacy of tranexamic acid in pediatric craniosynostosis surgery: a double-blind, placebo-controlled trial. Anesthesiology 2011;114:862-71.
2. Dubey SP, Schick B. Juvenile Angiofibroma. Cham, Switzerland: Springer, 2017.
-
 GA2-63 Image 1
GA2-63 Image 1
Top










