
AET-27
Use of C–MAC® video laryngoscope for intubation during ex utero intrapartum treatment for a neck mass involving upper airway.
Arteaga A, Guevara J, Marroquin M
Clinica Colombia, Bogotá D.C., Cundinamar, Colombia
Introduction
Ex utero intrapartum treatment (EXIT) procedure is mainly indicated to secure the airway of fetuses with antenatal diagnosis of oropharyngeal or neck masses, airway obstruction and facial malformations, while fetal oxygenation is maintained by uteroplacental circulation. Fetal intubation can be difficult in this scenario; direct laryngoscopy and other airway devices have been used to optimize visualization of the glottis. Our purpose is to document our experience successfully intubating a newborn with a C-MAC® video laryngoscope during an EXIT procedure.
Clinical Findings
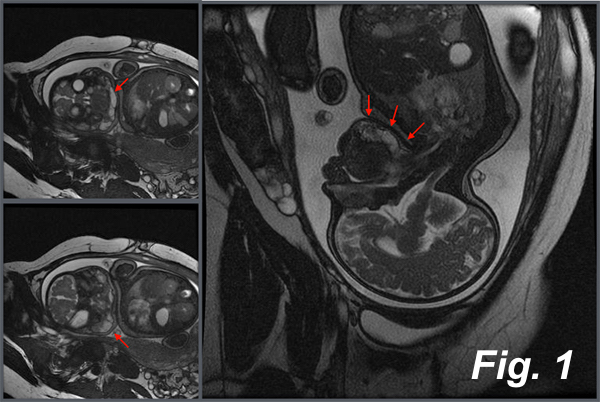
A healthy 26-year-old primiparous, had her fetus diagnosed with a neck mass involving the suprahyoid region suggestive of a lymphovascular malformation (Fig 1). With this clinical information, a multimodal team planned an EXIT procedure at 36w of gestation.
Anesthetic Intervention
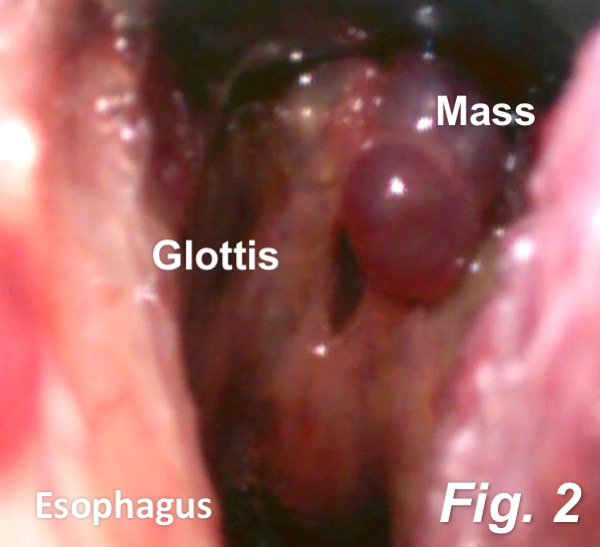
A general anesthetic was performed ensuring adequate uterine relaxation. The head of the fetus was partially delivered exposing the airway for assessment. Facial edema and mouth involvement was evident. Using a C-MAC® video laryngoscope with a C-MAC® Miller#1 blade we obtained a good laryngoscopic view which showed tongue and epiglottis involvement (Fig 2). A first attempt to intubate was made with a 3.0 uncuffed endotracheal tube on a guide wire, which failed because we encountered resistance while advancing the tube. To solve this situation, a sterile 8.0Fr Frova introducer was positioned into the space between the cords under video laryngoscopic view and subsequently it was possible to intubate the patient.
Time to a positive capnography was 7 min 56 sec. The umbilical cord blood gases showed no major impact on the newborn.
Discussion
EXIT procedure has concise indications. It transforms a potentially fatal neonatal airway emergency into a controlled scenario. The use of a video laryngoscope in this setting. is considered an innovative approach and to our knowledge there is only one case reported using a Glidescope®. Nonetheless, the use of C-MAC® video laryngoscope in this scenario has not been documented.
Our experience using traditional approaches for intubating newborns during EXIT procedures has proved multiple technical difficulties, mainly because of the limited fetal exposure. Given the fact that the C-MAC omits some of these issues, it allows a better view decreasing the intubation time.
Conclusion
The use of C-MAC® video laryngoscope for intubation during an EXIT procedure is a feasible option to achieve a successful endotracheal intubation.
References
1.Hoagland M. Anesthesia for fetal surgery. Pediatric Anesthesia, 27 (2017) 346–357.
-
 AET-27 Image 2
AET-27 Image 2 -
 AET-27 Image 1
AET-27 Image 1
Top










