
GA2-62
Anesthetic Management of a Neonate with Jeune Sydnome
Genis A, Salik I, Barst S
NYMC/Westchester Medical Center, Valhalla, NY, USA
Introduction:Jeune syndrome, also known as asphyxiating thoracic dystrophy, is a rare autosomal recessive chondrodysplasia that presents multiple challenges to the anesthesiologist. Although it often presents with abnormalities including thoracic and lung hypoplasia, there are other factors to consider when anesthetizing patients with this disorder. We present a 7-day old infant with Jeune syndrome that underwent brain imaging via an MRI to evaluate a cerebral cyst.
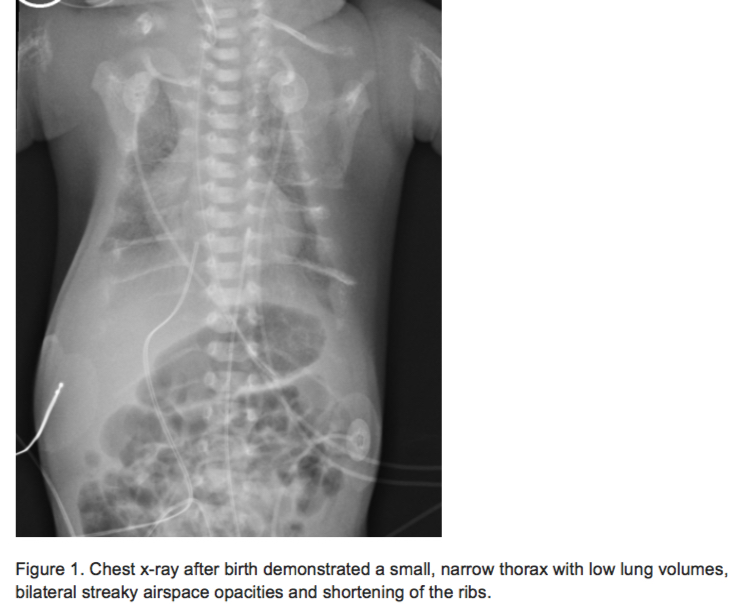
Case Presentation: The patient was twin B of a dizygotic twin gestation born at 36 weeks via C-section. Intrauterine growth restriction was noted during pregnancy and the neonate was born weighing 1870 grams. At birth there was minimal respiratory effort and Apgar scores were 3, 6, and 7 at 1, 5 and 10 minutes respectively, necessitating endotracheal intubation. Imaging demonstrated a narrow thoracic cage with small lung volumes (figure 1) and various skeletal deformities (figure 2). The patient also had documented renal dysplasia, respiratory distress syndrome and pulmonary hypertension. An echocardiogram demonstrated increased right ventricular systolic pressure. The patient remained on mechanical ventilation via a 3.0 uncuffed endotracheal tube when presenting for the MRI. Induction with sevoflurane commenced after standard ASA monitors were placed; anesthesia was maintained with volatile agents at 0.8 MAC and no other IV medications were administered. Pressure-controlled mechanical ventilation was utilized to deliver low tidal volumes to minimize airway pressures. The procedure was completed without complications and the patient remained intubated.
Discussion:Asphyxiating thoracic dystrophy is a rare genetic disorder that usually presents at birth with lung hypoplasia and restrictive lung disease. This leads to variable degrees of respiratory insufficiency and recurrent pulmonary infections that often result in respiratory failure and death in infancy. Patients often have small lung volumes, decreased functional residual capacity and decreased airway compliance. Intra-operatively, high airway pressures should be avoided, and low tidal volumes with increased inspiratory time are preferred to prevent barotrauma and the development of a pneumothorax. Lung hypoplasia can result in pulmonary hypertension with subsequent cardiac involvement. These children exhibit numerous systemic manifestations including skeletal deformities such as irregular epiphyses and short long bones, requiring careful intraoperative positioning to avoid nerve injury. They can also suffer from hepatic, pancreatic, bile duct and renal anomalies leading to cirrhosis and renal failure. Low doses of anesthetic drugs should be administered secondary to impaired hepatic and renal function.
Conclusion: Jeune syndrome is a complicated medical diagnosis associated with multiple anomalies. Anesthetic management of these patients should take into account the numerous systemic manifestations of their disorder.
-
 GA2-62 Image 1
GA2-62 Image 1
Top










