
AIR-12
Stylet Mishap in a Patient with a Known Difficult Airway
Teen M, Jiminez N
Cincinnati Children's, Cincinnati, OH, United states
This is a case of a 6 week-old 3.3 kg premature male infant with a constellation of malformations including a recently repaired coarctation of aorta, dysmorphic features, micrognathia, arthrogryposis, vocal cord paralysis, tracheomalacia and a known difficult airway, who was found to have pyloric stenosis and is scheduled for a laparoscopic pyloromyotomy. He has had to be intubated emergently twice prior to this surgery, requiring multiple attempts by the ICU and ENT teams. The best view obtained was a Grade 3 with direct laryngoscopy (DL) using a Miller 1 blade and “limited vocal cord visualization with C-Mac Miller 1â€.
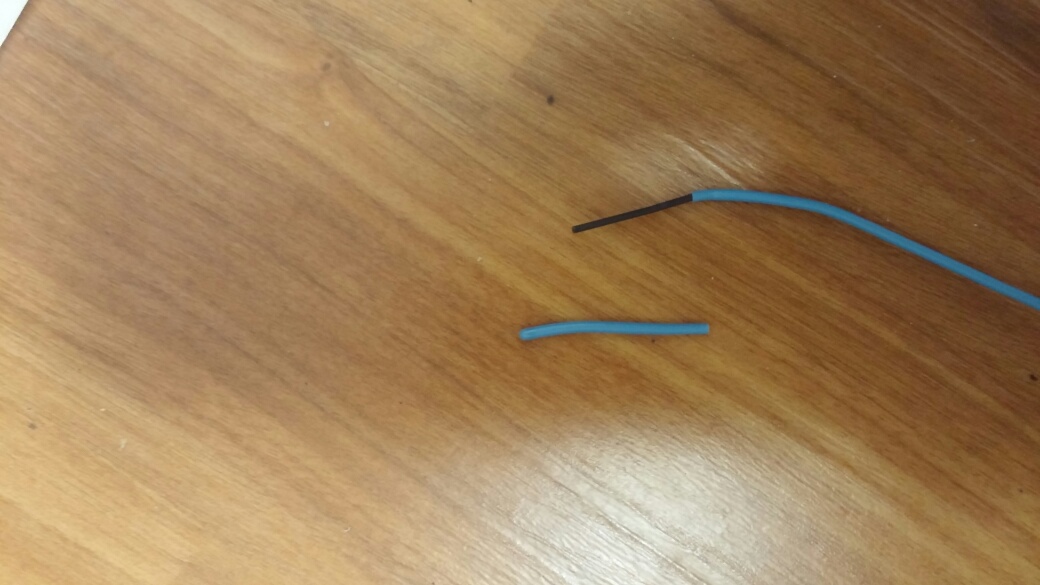
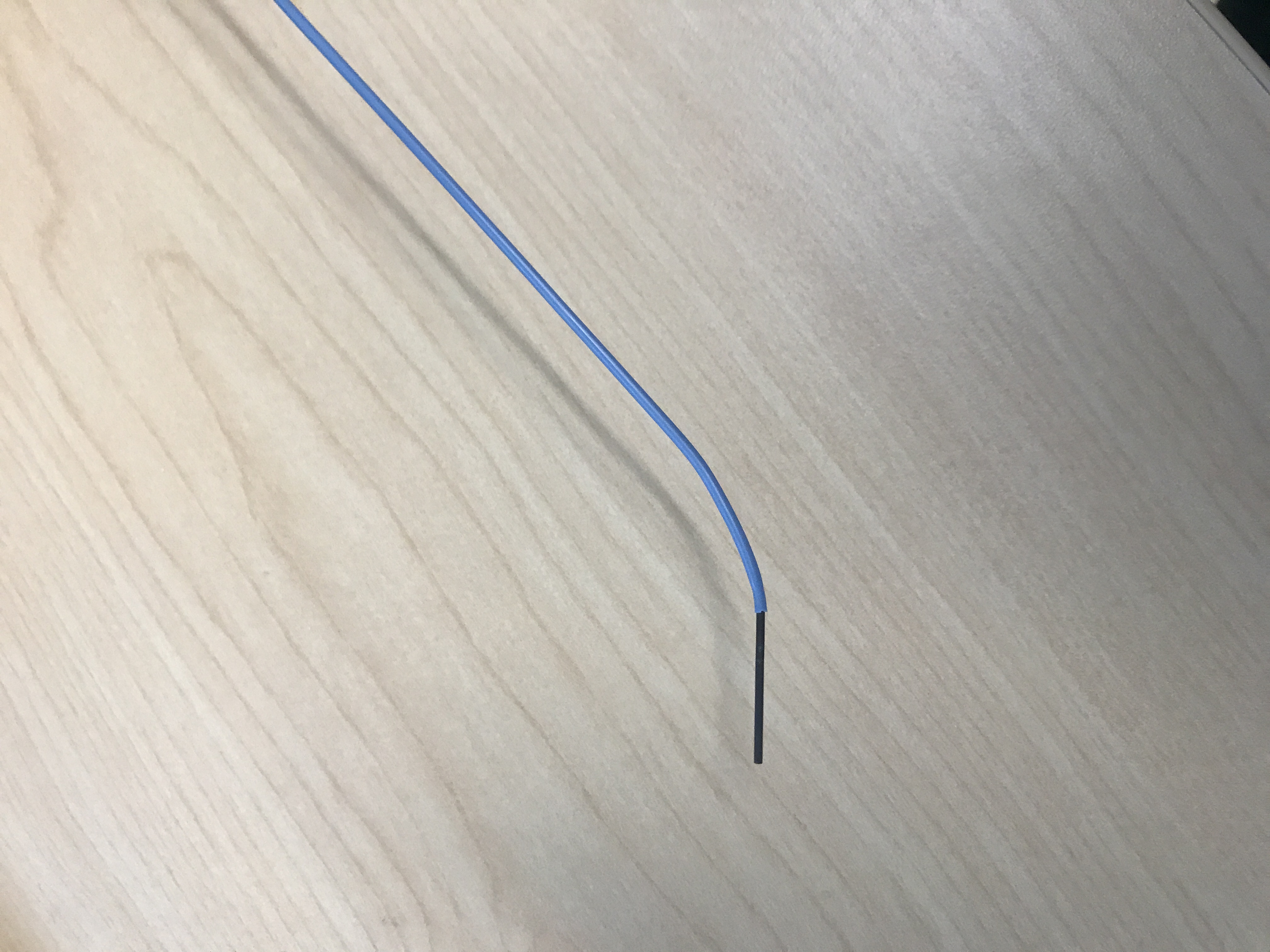
He is transported from the PICU still intubated from the last emergent intubation. It is reported to be a “blind†intubation by ENT after 7 attempts by the PICU team. However, he has a 3.0 uncuffed endotracheal tube (ETT) in place with a leak at 10 cmH2O. This is determined to be inadequate for the laparoscopic procedure. The decision is made to reintubate his airway with a cuffed ETT in the OR with ENT present. In a controlled fashion, following the path of the current ETT, a Grade 2 view is obtained via DL with a Miller 1 blade. The ETT is removed and a styletted cuffed 3.0 ETT is inserted pass the vocal cords. The stylet is then removed with a lot of resistance. The tip of the stylet is noted to be unusual (as pictured). The blue coating of the stylet is thought to be stuck within the ETT lumen, and hopefully, not in the patient’s airway.
Positive pressure ventilation (PPV) through the ETT is not initiated. Instead, the ETT is removed and he is mask ventilated easily while a new ETT is styletted. The blue coating of the stylet is noted in its entirety in the lumen of the removed ETT. A cuffed ETT is then inserted via DL uneventfully.
This case reminds us the importance of recognizing patients with difficult airway, communicating and documenting it appropriately. The decision to exchange the ETT was a difficult one with the known history of difficult intubation in a small infant. In a laparoscopic case, it would be impossible to achieve adequate ventilation with a significant leak around an uncuffed ETT. We discussed alternative ways of exchanging the ETT without losing the airway, but there are not many options in a small airway, besides having ENT present as backup. Lastly, timely recognition of equipment malfunction is vital in this case. We were fortunate to have noticed the loss of coating of the stylet tip prior to PPV initiation. PPV could have forced the foreign body into the patient’s tracheobronchial tree, obstructing the airway, and further complicating this patient’s already complex history.
-
 AIR-12 Image 2
AIR-12 Image 2 -
 AIR-12 Image 1
AIR-12 Image 1
Top










