
NM-347
Defining the incidence of perioperative transfusion-related pulmonary complications in pediatric non-cardiac surgical patients
Thalji L, Thum D, Weister T, Webber W, Stubbs J, Kor D, Nemergut M
Mayo Clinic, Rochester, MN, USA
Introduction: Transfusion-related acute lung injury (TRALI) and transfusion-associated circulatory overload (TACO) are the leading causes of transfusion-related fatalities. While these transfusion related pulmonary complications (TRPCs) have been well detailed in adults, their burden in pediatric patients remains poorly defined. We sought to delineate the incidence and epidemiology of TRALI and TACO following intraoperative blood product administration in pediatric patients.
Methods: We evaluated all consecutive pediatric patients (age <18 years) who received intraoperative blood product transfusions during non-cardiac surgeries between January 2010 – December 2014. Exclusion criteria were congenital cyanotic heart disease, evidence of preoperative respiratory insufficiency, extracorporeal membrane oxygenator requirement, and intraoperative demise. Medical records were electronically screened to identify those with both evidence of hypoxemia (PaO2:FiO2 ratio <300 mmHg, oxygenation index >4 mmHg, oxygen saturation <90%, or an oxygen requirement after postanesthesia care unit dismissal), and in whom a chest x-ray was obtained within 24-hours of surgery. Records were then manually reviewed by two independent physicians to determine whether they met diagnostic criteria for TACO or TRALI. Disagreement was adjudicated by a third senior physician.
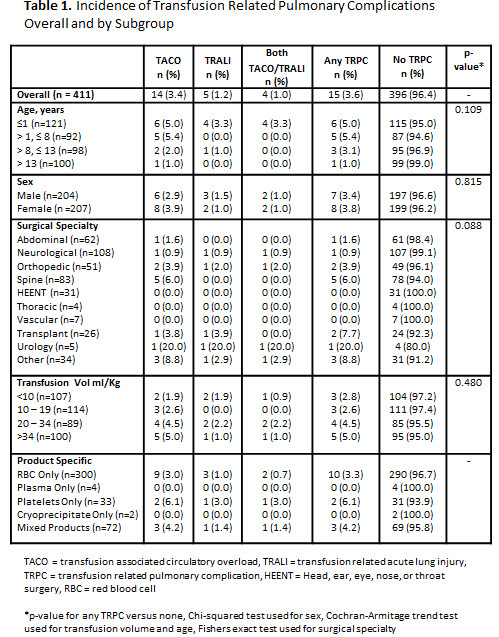
Results: In our cohort of 411 patients, the incidence of TRPCs was 3.6%. TACO occurred in 3.4% of patients, TRALI was identified in 1.2%, and 1% had evidence for both TRALI and TACO. Overall incidence rates were similar between males (3.4%) and females (3.8%, p=0.815). Although a trend towards an increased incidence of TRPCs was observed in younger patients, this did not reach the threshold for statistical significance (p=0.109). The incidence of TRPCs was comparable across all subsets of transfusion volume (p=0.184), and surgical specialties (p=0.088). Among the 15 patients experiencing TRPCs, RBCs were administered to 13 subjects, plasma to 3, platelets to 3, cryoprecipitate to 2 and autologous blood to 3. Three patients with TRCPs were transfused mixed blood components.
Discussion: TRPCs occurred in 3.6% of transfused pediatric surgical patients with the majority of cases attributable to TACO - congruent with adult literature. The frequency of TRPCs was comparable between genders, and across various surgical procedures and transfusion volumes. The observed trend towards increased TRPCs in younger children warrants further consideration in future investigations. RBC administration was the associated component for the majority of TRPCs, although platelets demonstrated the highest risk per component transfused.
Conclusion: The incidence of TRPCs in pediatric patients is similar to estimates derived from adult populations. Mitigation of perioperative TRPCs in pediatric patients is reliant upon studies powered to examine patterns and predictors of this highly morbid entity.
-
 NM-347 Image 1
NM-347 Image 1
Top










