
OS1-135
Does Use of Tranexamic Acid Reduce Blood Loss in Pediatric Patients Undergoing Pelvic Osteotomy?
Lazo T, Chidambaran V, Keyes S, Ihnow S, Whitlock P, McCarthy J, Tamai J, Ding L
Cincinnati Children's Hospital, Cincinnati, OH, US
INTRODUCTION
Dysplastic hips in children with cerebral palsy often require reconstructive hip surgeries in the form of femoral and/or pelvic osteotomies, which can result in marked blood loss due to the high vascularity of the bone and inability to use tourniquets. 1 This increases the likelihood of blood transfusion and associated risks. Thus, measures to decrease blood loss are necessary. Tranexamic acid (TXA) is a plasminolytic inhibitor that is effective in reducing blood loss in adults undergoing total hip arthroplasty.2 Although TXA is used in pediatric spinal and craniosynostosis surgeries, there are no studies evaluating the use of TXA in pediatric femoral and pelvic osteotomies. In this study, we evaluated the efficacy of TXA in decreasing blood loss in pediatric patients undergoing pelvic and femoral osteotomies, theorizing that the use of TXA would reduce associated blood loss and need for transfusions.
METHODS
We conducted a retrospective chart review of children <18 years with a diagnosis of hip dysplasia, hip dislocation and/or hip subluxation who had 2 or more pelvic or femoral osteotomies between Jan 1, 2011 and Jan 31, 2017. Patients undergoing periacetabular osteotomies were excluded. We identified 116 patients who met the inclusion criteria; 51 received standardized doses of TXA. Data collected included demographics, type of procedure, diagnosis, pre- and post-operative hemoglobin, estimated blood loss (EBL), cell saver volume, blood products transfused, and complications. Univariate analysis was used to examine variables between the groups, and those significant at p<0.1 were included in multiple regression. Our primary outcome was percent blood loss (EBL/estimated blood volume by weight) and our secondary outcome was need for transfusion.
RESULTS
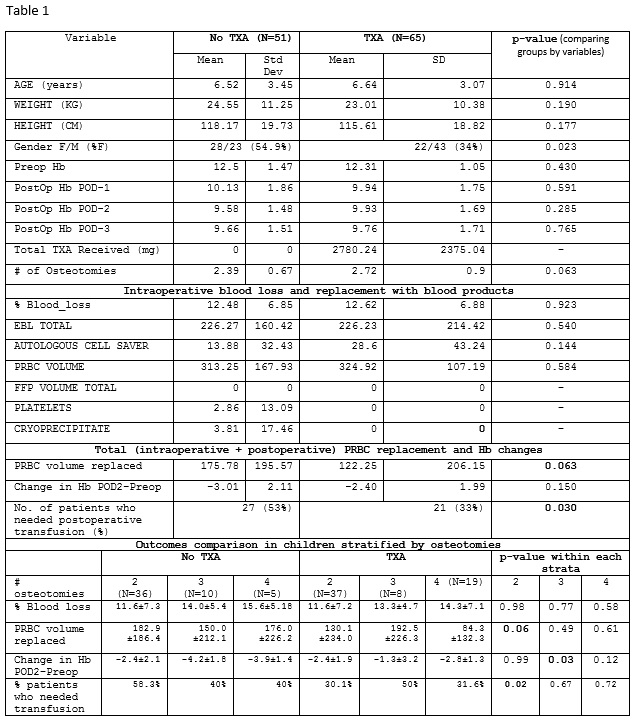
Data for TXA/no TXA group comparisons are presented in Table 1. The use of TXA did not decrease the % blood loss (p=0.923) but did decrease need for blood transfusions perioperatively (p=0.030). In addition, children having >2 osteotomies had significantly higher % blood loss compared to 2 osteotomies (11.6±7.2% vs. 14.2±6.0%, p=0.023). In children who had >2 pelvic osteotomies who did not receive TXA, incidence of transfusions was higher (58.3% vs 30.6%; p=0.017), and they had a greater decrease in hemoglobin, from pre-op to post-op values (-4.1±1.7 vs. -2.4 ± 2.1; p=0.013), compared to those who received TXA.
CONCLUSIONS
The use of TXA resulted in decreased need for blood transfusions in children undergoing pelvic osteotomies, with a bigger difference in those undergoing >2 pelvic osteotomies. These findings suggest TXA might be a useful agent against blood loss in this cohort. Prospective studies in larger cohorts are warranted to optimize TXA dosing and could include genetic screening for efficacy.
REFERENCES
1. http://arizona.openrepository.com/arizona/bitstream/10150/603585/9/Arthur_Poster.pdf
2. Henry, D. A., (2011). Cochrane Database Syst Rev 19(1).
-
 OS1-135 Image 1
OS1-135 Image 1
Top










