
CR1-178
Anesthetic Management of Thoracoscopic Posterior Tracheopexy – a novel approach to severe tracheomalacia
1Masaracchia M, 2Dewberry L, 1Wine T, 1Somme S, 1Janosy N
1Children's Hospital Colorado, Aurora, CO, USA; 2University of Colorado, Aurora, CO, USA
Introduction
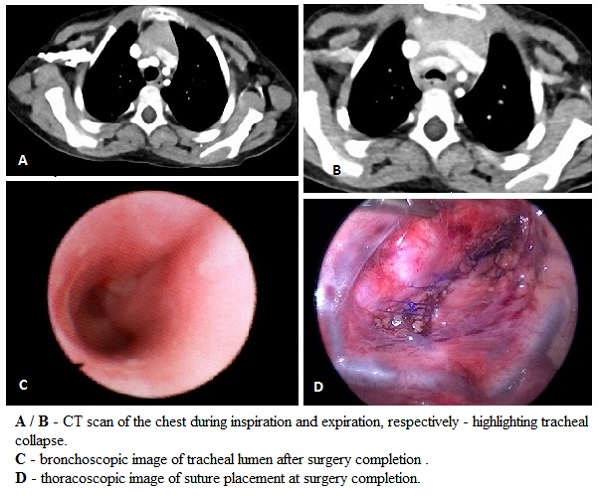
Tracheomalacia results from a reduction in elastic fibers or impaired cartilage integrity and leads to increased tracheal collapsibility. Normal physiologic airway narrowing that occurs during expiration in response to high intrathoracic pressures is accentuated, and can cause clinically significant obstruction. External compression can also occur from the aorta anteriorly and the esophagus posteriorly. The severity of symptoms dictates treatment. Thoracoscopic posterior tracheopexy is a novel approach that involves stenting the trachea by attaching its posterior aspect to the anterior longitudinal spinal ligament under guidance of fiberoptic bronchoscopy (FOB).
We describe the management of a complex 13.5 kg, 3-year-old female with severe tracheomalacia who was scheduled for correction by posterior tracheopexy. Her medical history was significant for a chromosomal deletion syndrome (46XX del 2q37.1), cervical subluxation, hydrocephalus and subsequent VP shunt placement, obstructive sleep apnea on BiPAP, and chronic lung disease on oxygen (1L/min O2 NC). CT imaging demonstrated significant narrowing (53%) of the tracheal AP diameter at the level of the brachiocephalic artery.
Anesthetic Management
An inhalational induction was performed and immediately transitioned to a total intravenous anesthetic for monitoring of somatosensory evoked potentials (SSEP). She was intubated with a cuffed 3.5 ETT, and a 5F Arndt endobronchial blocker (AEB) was placed extraluminally into the right main stem bronchus for lung isolation. An orogastric tube was placed to aid in surgical identification of the esophagus. The patient was positioned in the lateral decubitus position for a right thoracoscopy. Endoluminal FOB was used to assist in suturing the posterior trachea to the anterior spinal ligament. She remained hemodynamically stable throughout, SSEPs were intact, and she was extubated to BiPAP at the end of the procedure.
Discussion
Thoracoscopic posterior tracheopexy is a relatively novel approach performed as an alternative to thoracotomy. This minimally invasive technique is advantageous for patients with already compromised respiratory mechanics. However, the need for operative FOB guidance and simultaneous lung isolation makes for a challenging anesthetic. Endobronchial intubation was not an option because tracheal FOB guidance was needed for surgical correction. Endoluminal placement of AEB was not feasible secondary to ETT size and the need for fiberoptic guidance. This case highlights a unique need for one lung ventilation in the setting of operative FOB guidance, and how both can be successfully achieved by the extraluminal placement of a bronchial blocker.
References
Shieh HF, Smithers CJ, et al. Posterior tracheopexy for severe tracheomalacia. J Pediatr Surg. 2017; 52(6): 951-955.
-
 CR1-178 Image 1
CR1-178 Image 1
Top










