
NM-203
Itching for an answer: should sugammadex be given for suspected vecuronium anaphylaxis?
1Simpao A, 2Puglia II M, 1Galvez J, 1Jablonka D
1The Children's Hospital of Philadelphia, Philadelphia, PA, USA; 2University of Michigan, Mott Children's Hospital, Ann Arbor, MI, USA
Case presentation:
A 32 month-old male presented for an urgent ventriculoperitoneal (VP) shunt revision. His history was significant for 4th ventricle oligodendroglioma related hydrocephalus which required, in addition to the tumor resection, multiple interventions to maintain patency of his shunt. He had no previous anesthesia related problems.
The child looked mildly obtunded in the holding area despite adequate fluid resuscitation.
Upon arrival to the OR, he turned agitated and tearful. We provided inhalation induction with sevoflurane followed by a fentanyl 2 mcg/kg, and vecuronium 0.1mg/kg bolus once adequate ventilation via mask was confirmed.
Ventilatory compliance decreased during mask ventilation and then ventilation was impossible through a well secured endotracheal tube, His skin turned dusky and gray.
No pulse was palpable. Help arrived, and the team provided chest compressions.
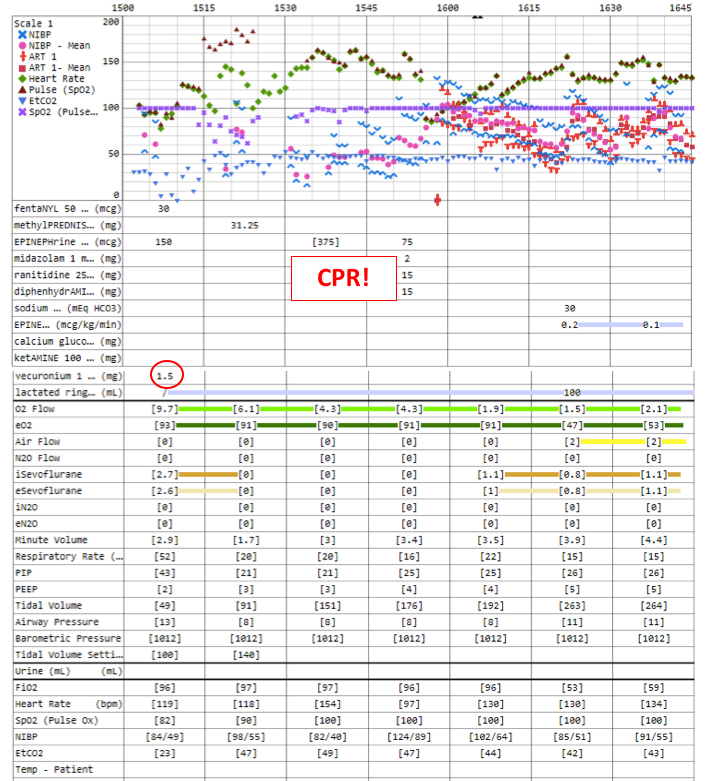
Peripheral pulsations re-appeared approximately 20 minutes after repeated doses of epinephrine (fig.1). An arterial blood gas revealed profound metabolic acidosis. The team at this point suspected severe anaphylaxis.
This child tolerated the procedure and fully recovered from this event with no neurologic sequelae. However, his VP shunt needed to be revised again a week later. Consultation with an allergy specialist became critical.
Laboratory results: Tryptase level 58.1 ug/L (normal <10), skin prick test highly positive for vecuronium but not rocuronium.
Discussion:
Neuromuscular blockers (NMB's) account for the majority of anesthesia related anaphylaxis. Treatment in the operating includes early recognition, immediate discontinuation of the offending agent, epinephrine, fluid resuscitation, and histamine receptor blockers. An elevated tryptase level indicates mastocyte degranulation and usually confirms the diagnosis.
Sugammadex has been previously described in the treatment of aminosteroid NMB related anaphylaxis. Its mechanism of action involves encapsulating rocuronium or vecuronium with rapid clearance from the circulation.
The presence of offending agents (e.g., rocuronium or vecuronium) at the basophil surface in a cross link with IgE antibodies triggers and sustains the release of inflammatory and vasomodulation substances (1). Thus, the removal of the offending agent is one of the cornerstones of anaphylaxis management.
The authors did consider administering sugammadex, but we opted not to do so given its recent introduction into our formulary and our limited experience using this drug in pediatric patients.
As sugammadex gains widespread adoption in the US, particularly in our field, we expect more debate regarding this particular therapeutic indication.
1. Baldo BA et al. Drug-specific cyclodextrins with emphasis on sugammadex, the neuromuscular blocker rocuronium and perioperative anaphylaxis: implications for drug allergy. Clin Exp Allergy. 2011;41:1663-78.
-
 NM-203 Image 1
NM-203 Image 1
Top










