
OS2-142
Coagulopathy after Major Pediatric Trauma and Resultant Outcomes- a Retrospective Study
1Ibekwe S, 2Austin T, 2Williamson J, 2Guzzetta N
1Johns Hopkins Hospital, Baltimore, MD, United states; 2Emory University School of Medicine/Children's Healthcare of Atlanta, Atlanta, GA, United states
Introduction
Trauma is the leading cause of death in children (1), and coagulopathy is a well-documented component of trauma. Pediatric anesthesiologists are often involved in the medical care of pediatric trauma victims, either in the emergency department (ED) during resuscitation or the operating room (OR) during emergency surgery. In adult trauma victims, coagulopathy present on admission is associated with poor outcomes (2). Unfortunately, similar data in the pediatric population is sparse. Thus we performed a retrospective study to analyze the relationship between coagulopathy upon presentation to the ED and clinical outcomes in pediatric trauma victims at a major urban tertiary care, level I trauma center.
Methods
After IRB approval, we retrospectively reviewed the medical records of all pediatric trauma victims who presented to Children’s Healthcare of Atlanta between 1/9/2014 and 8/3/2016. Inclusion criteria were age ≤18 years and an Injury Severity Score (ISS) ≥15 on presentation to the ED. Multiple variables were collected at the time of presentation. Clinical outcomes included duration of mechanical ventilation, intensive care unit (ICU) length of stay (LOS) and in-hospital mortality. In our statistical analysis, two separate linear regressions were performed with duration of mechanical ventilation and ICU LOS set as the response variables. Initially, 14 explanatory variables were selected for analysis. Due to the concern that some variables were correlated to one another, variable selection occurred through the use of an elastic net algorithm with the shrinkage parameter (ï¬) set to its minimum. The duration of mechanical ventilation and ICU LOS were log transformed for the final regression models to satisfy model assumptions. A two-tailed p<0.05 was considered significant.
Results
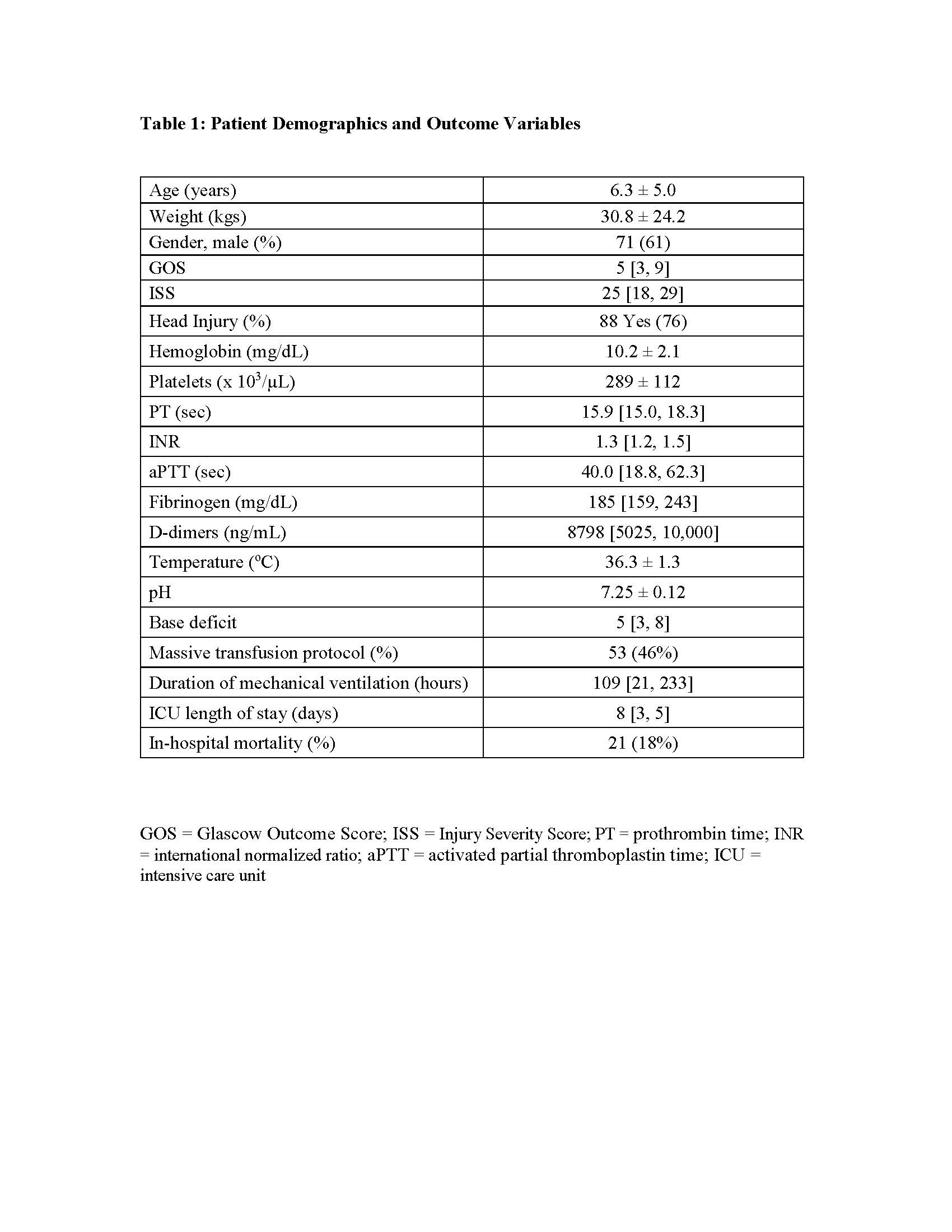
One hundred sixteen patients were included in our final analysis. A summary of all collected variables is shown in Table 1. The only variable associated with log ventilation time was the Glascow Outcome Score (GOS). aPTT, d-dimers, GOS, and pH were associated with log ICU LOS.
Conclusion
The variable most predictive of clinical outcome, i.e. duration of mechanical ventilation and ICU LOS, after pediatric trauma was the GOS. In terms of coagulation parameters, the aPTT and presence of d-dimers on admission were associated with an increased ICU LOS. Other investigators have also shown that fibrinolytic dysregulation is associated with poorer outcomes in pediatric trauma (3). Together, these findings indicate that antifibrinolytic therapy may benefit pediatric trauma victims. Further clinical studies are needed to determine the validity of this hypothesis.
References
1. J Pediatr 2012;160:204
2. J Trauma 2003;55:39
3. Ann Thorac Surg 2017;266:3
-
 OS2-142 Image 1
OS2-142 Image 1
Top










