
NM-234
Intraoperative serratus anterior block for post-operative pain control after pediatric thoracotomy: a historical cohort study.
1Bunnell A, 2Hagen J, 2Kars M, 2Barnett N
1Hofstra University - Northwell School of Medicine, New Hyde Park, NY, United states; 2Long Island Jewish Medical Center at Northwell Health, New Hyde Park, NY, United states
Introduction:
Thoracotomies result in substantial postoperative pain. Varying techniques have been described for postoperative pain control in adult patients, including thoracic epidural, paravertebral block, and serratus anterior block (SAB). The SAB is a relatively new technique said to be a safe and effective alternative to epidural anesthesia in adults. While regional techniques have been shown to be safe and their use encouraged in pediatrics, the SAB has not been well described for children. We sought to examine the efficacy of the SAB as part of a multimodal regimen in pediatric patients undergoing thoracotomy.
Methods:
We reviewed charts of 18 children ages 5 days to 15 years, who underwent thoracotomy between September 2012 and September 2017, cared for by a sole pediatric anesthesiologist. Patients were undergoing surgery related to congenital cardiac and pulmonary diagnoses. We compared those that received pre-incision SAB (n=10) to those that did not (n=8). The primary outcome was narcotic administration. Secondary outcomes included total anesthesia time, surgical time, time to opioid rescue, and time to discharge. Data was analyzed using a two-tailed t-test.
Results:
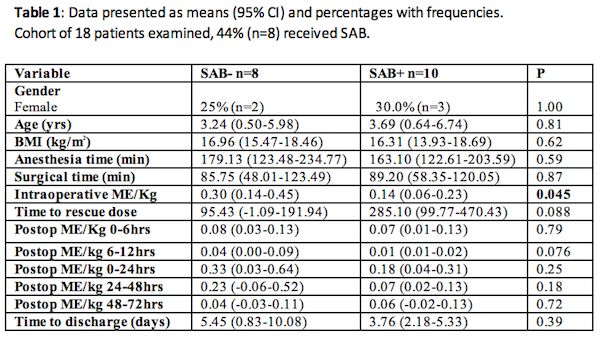
Table 1: Data presented as means (95% CI) and percentages with frequencies.
Intraoperative narcotic administration was significantly reduced in patients who underwent SAB, with a mean of 0.14 mg/kg of morphine equivalent versus 0.30 mg/kg (p<0.05). Time to first rescue dose (285.10min for SAB+ versus 85.75min for SAB-, p=0.088), and postoperative narcotic administration at 6-12hours (0.01mg/kg for SAB+ versus 0.04mg/kg for SAB-, p=0.076) indicate a trend. There were no complications related to the SAB.
Discussion:
Pre-incision SAB for thoracotomy was associated with less intraoperative narcotic administration compared to children who did not receive SAB. We also demonstrated a trend towards decreased postoperative narcotic administration overall, but especially at 6-12 hours. While clearly limited by sample size, our study shows good promise for the SAB as part of a multimodal regimen in pediatric patients undergoing thoracotomy.
Conclusions:
Though our study did show a decrease in intraoperative narcotic administration associated with the SAB, the power of our study was greatly limited by sample size, and we suspect that future research will demonstrate greater efficacy of the SAB.
References:
1. Khalil A, et al. Ultrasound-Guided Serratus Anterior Plane Block Versus Thoracic Epidural Analgesia for Thoracotomy Pain. Journal of Cardiothoracic and Vascular Anesthesia 2016.
2. Blanco R, et al. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia 2013;68:1107-1113
3. Polaner D, et al. Pediatric Regional Anesthesia Network (PRAN). Anesthesia & Analgesia 2012;115:1353-1364.
4. McPherson M. Demystifying opioid conversion calculations. Bethesda, MD: American Society of Health-System Pharmacists, 2009.
-
 NM-234 Image 1
NM-234 Image 1
Top










