
GA1-47
Comparison of blood pressure measurements in upper and lower extremities in children under general anesthesia
1Hayes S, 1Syed F, 1Patel A, 2Kadah K, 2Adan S, 1Miketic R, 1Sebastian R, 1Winch P, 1Tobias J, 2Wani T
1Nationwide Children's Hospital, Columbus, OH, United states; 2King Fahad Medical City, Riyadh, Riyadh, Saudi arabia
Introduction: During surgery, blood pressure can be obtained non-invasively (NIBP) by oscillometry or invasively (IBP) by an arterial cannula. Limited data exist comparing NIBP to IBP measurements in anesthetized children, but a tendency towards falsely elevated NIBP values has been reported in newborns. With BP guiding major therapeutic decisions in the perioperative area, inaccuracies may complicate the timely diagnosis and treatment of hypotension. We are performing a prospective observational study to further evaluate clinically significant errors in NIBP relative to IBP measurements. Our secondary aim is to investigate the consistency of upper versus lower extremity NIBP.
Methods: Patients under 10 years of age, ASA 1-3, were enrolled in our study if they were to receive general anesthesia with a planned arterial cannula. NIBPs were measured with two separate oscillometers of the same make with appropriately sized BP cuffs. Mean arterial pressures (MAP) from 3 sites (radial artery, arm cuff, and leg cuff) were recorded at 5 minute intervals for 10 readings per patient. The primary outcome was deviation of MAP >5 mmHg between IBP and at least one NIBP at any point during the study.
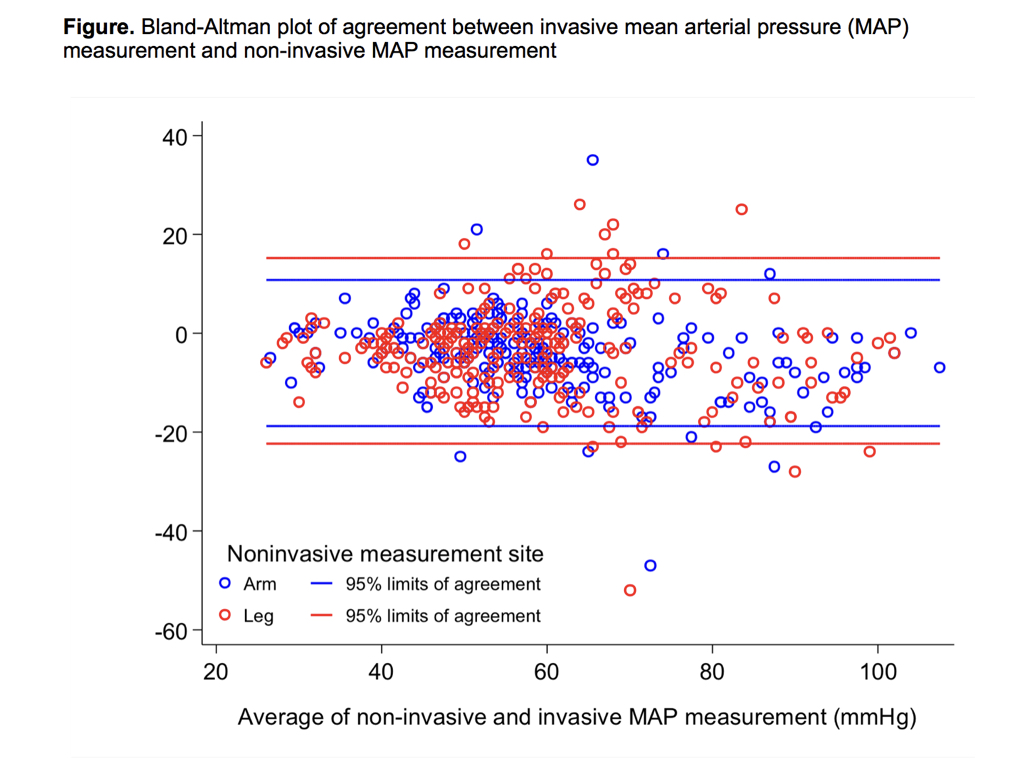
Results: We have enrolled 13 boys and 12 girls to date, ages 0-4 years. Across all data points, MAP was 57 ± 15 mmHg at the arm, 57 ± 16 mmHg at the leg, and 61 ± 17 mmHg via the arterial cannula. IBP and NIBP measurements generally demonstrated good concordance (Figure). In 24 of 25 patients, IBP deviated by >5 mmHg at least once from either the arm or the leg. In 13 patients (52%; 95% confidence interval: 32%, 72%), arm or leg NIBP over-estimated MAP by >5 mmHg at one or more time points. Across all data points, leg and arm MAP measurements did not show significant bias (difference: 0.5 mmHg [95% CI: -1, 2]; paired t-test p=0.385; Bland-Altman 95% limits of agreement: -16, 17 mmHg). No difference was noted in the accuracy of the NIBP when comparing the arm and leg measurements.
Discussion: Previous studies comparing NIBP to IBP measurements in anesthetized children are limited and have been largely inconclusive in terms of degree of BP mismatch. Our preliminary results suggest NIBP and IBP generally correlate well, but clinically significant discrepancies using NIBP occurred one or more times during the study period (10 BP measurements or approximately 50 minutes). Although there was no consistent trend in over or under measuring MAP by NIBP, our findings suggest caution is necessary when using NIBP monitoring to avoid medical mismanagement. The results also highlight the importance of using additional intraoperative monitors such as electrocardiography, pulse oximetry, and capnography to corroborate BP values when NIBP monitoring is used.
Conclusion: The frequency of clinically significant NIBP deviation supports the importance of invasive BP monitoring when hemodynamic fluctuations would be particularly detrimental.
-
 GA1-47 Image 1
GA1-47 Image 1
Top










