
NM-375
Cost-effectiveness of “Fast Computerized Tomography (CT)†in pediatric cardiac patients: the impact of general anesthesia
1Wise-Faberowski L, 1Irvin M, 2Velasquez N
1Stanford University/Lucile Packard Children's Hospital, Palo Alto, CA, USA; 2University of Pittsburg, Pittsburgh, PA, USA
Background:
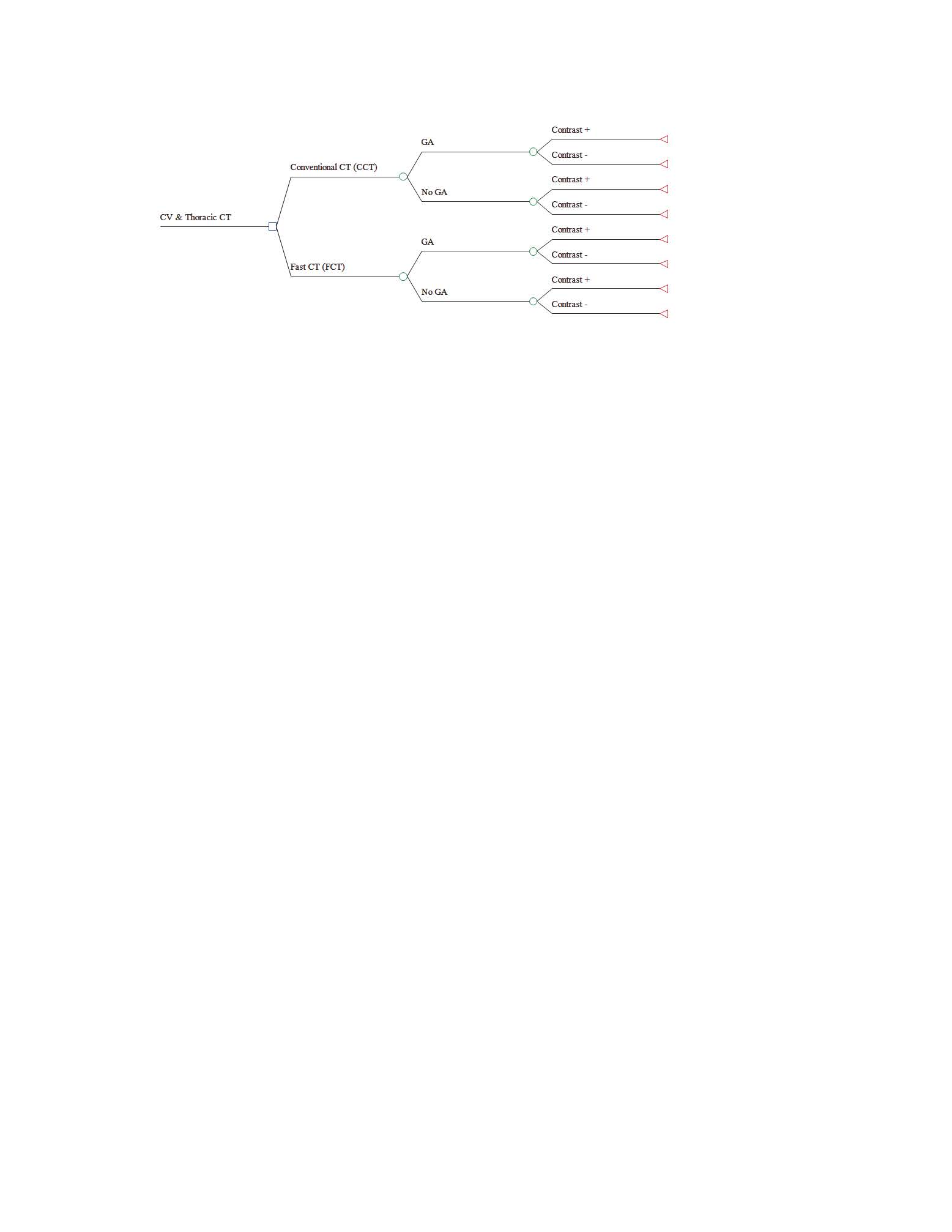
Anesthetic neurotoxicity is a continued concern. Efforts to limit anesthetic exposure, in not only children with congenital heart disease but all children, is an objective goal for not only anesthesiologists, but institutions as well. New generation computerized tomography “Fast (CT) “ scanners allow faster imaging and increased success in imaging of uncooperative patients. As a result, they may decrease the use of sedation-general anesthesia and thus offset the cost of faster CT imaging devices. Our objective was to determine the cost-effectiveness of new generation “Fast CT†scanners versus conventional 64-slice CT scanners in reference to use of sedation-general anesthesia.
Methods:
Following IRB approval, Medical and administrative records of children with congenital heart disease, age ≤ 8 years, who underwent CT imaging between 2009 and 2015 on two different types of multi-slice CT scanners in an academic quaternary children’s hospital were retrospectively reviewed. Probabilities for undergoing sedation-general anesthesia and use of contrast material were calculated and used in a probabilistic cost-effectiveness model . Costs included hospital, professional, contrast material, and indirect cost elements from provider perspective with one episode of care time horizon. Sensitivity analyses were performed on key inputs including: probability of undergoing sedation-general anesthesia, costs of CT imaging using new generation “Fast CT†and conventional 64-slice CT scanner.
Results:
Rate of sedation-general anesthesia was 9% lower when imaging is performed with a new generation CT scanner. The probabilistic cost-effectiveness model calculated that in 1,000 CT imaging exams, 171 hours of sedation-general anesthesia would be saved at a decremented cost of $308,884. With the incremental cost of a new generation scanner not included, the cost-effectiveness ratio (ICER) of new generation CT scanner is -$1,844 per one hour of anesthesia time saved. At a willingness-to-pay of $2,500 per anesthesia hour saved, imaging with a new generation CT scanner remains cost effective up to an average cost threshold of $4,562 for a CT exam under sedation-general anesthesia (Figure).
Conclusion:
Children with congenital heart disease have repeated anesthetic exposure for multiple diagnostic procedures. As more institutions consider new strategies to limit anesthetic exposure in “at-risk†pediatric populations, many are faced with the costs of the new technology to achieve such goals. New generation “Fast CT†scanners reduce use of sedation-general anesthesia in CT imaging of children and saves resources with a favorable ICER. Since young age and underlying cardiac disease is a determining factor in the need for anesthesia/sedation for these procedures, institution selection by not only parents and referring physicians but also third-party payers to limit anesthetic exposure and it’s risk, may provide additional financial incentives for institutions to consider, as well.
-
 NM-375 Image 1
NM-375 Image 1
Top










