
GA4-81
Air and CSF: Two Uncommon Causes of Life-Threatening Abdominal Compartment Syndrome in Children
1McKeon D, 2Herbst M, 1Smith C, 1Kaminski E
1Children's Hospital of Michigan, Canton, Michigan, United states; 2University of Iowa Stead Family Children's Hospital, Iowa City, Iowa, United states
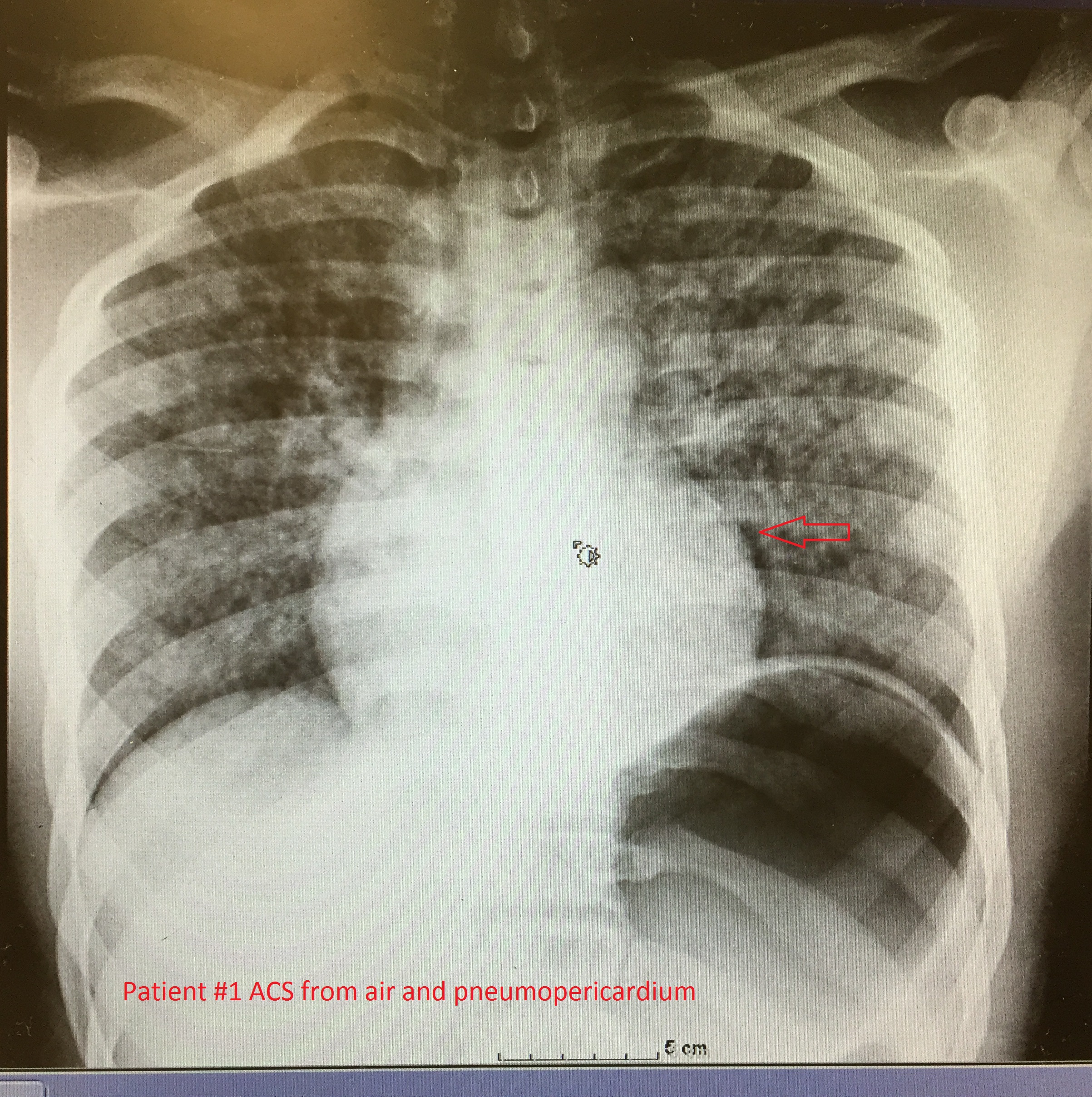
Abdominal compartment syndrome (ACS) is a rare but devastating complication in pediatrics with an associated mortality rate of 40-60%. ACS can be caused by a wide variety of conditions most commonly intra-abdominal pathology and sepsis requiring massive fluid resuscitation (1). We present two cases of ACS from atypical causes: one pneumoperitoneum due to tracheal rupture and one hydroperitoneum due to shunted cerebrospinal fluid (CSF). Both led to the inability to ventilate and subsequent cardiovascular collapse.
The first patient was a 4kg two month old male born at 29 weeks gestation with lung disease of prematurity and subglottic stenosis. During rigid bronchoscopy with tracheal balloon dilation, the patient became bradycardic and hypoxic. After confirmed endotracheal intubation, the patient was still unable to be ventilated. Pediatric Advanced Life Support (PALS) protocol was initiated. Bilateral needle thoracostomies were performed but these had no effect. Despite orogastric suctioning the patient’s abdomen became severely distended and tense. General surgery was emergently consulted and performed a decompressive laparotomy. Within seconds, spontaneous circulation returned.
The second patient was a 6kg two month old male born full term with congenital hydrocephalus who had undergone placement of bilateral subdural and ventriculo peritonal (VP) shunts at three weeks of age. He was readmitted with increasing abdominal distension and respiratory failure. Overnight he had increasing ventilatory requirements, decreased urine output and hemodynamic instability. Due to his worsening status, the decision was made to externalize the patient’s shunt emergently. Shortly after transport to the operating room, ventilation became extremely difficult and the patient became severely hypoxic and bradycardic. Cardiopulmonary resuscitation was initiated along with aggressive manual ventilation while the shunt was quickly externalized. Over one liter of CSF was aspirated from the abdomen with immediate return of easy ventilation, exhaled CO2, and spontaneous circulation.
The incidence of abdominal compartment syndrome among critically ill children is reported to be 0.6 to 10 percent; however, it is often under recognized by medical professionals (2). Our two cases demonstrate that abdominal compartment syndrome can occur from rapid accumulation of air from tracheal rupture and abdominal accumulation of CSF from a VP shunt and should remain in the diagnostic differential even when the most common risk factors are absent.
(1) E. Divarci, E and Karapinar, B et al. “Incidence and prognosis of intraabdominal hypertension and abdominal compartment syndrome in children,†Journal of Pediatric Surgery 51 (2016) 063.
503–507.
(2) Thabet, FC and Ejike, JC. “Intra-abdominal hypertension and abdominal compartment syndrome in pediatrics. A review,†Journal of Critical Care. October 2017Volume 41, Pages 275–282.
-
 GA4-81 Image 1
GA4-81 Image 1
Top










