
PR1-161
The Effect of CYP2D6 genotype on Oral Liquid Oxycodone Pharmacokinetics in pediatric patients
1Sriswasdi P, 2Dube C, 3Goobie S, 1Pereira L, 4Manzi S
1Boston Children's Hospital, Boston, MA, USA; 2Boston Children's hospital, Boston, MA, USA; 3Boston Children,s Hospital, Boston, MA, USA; 4Boston Chidren's Hospital, Boston, MA, USA
Introduction: Oxycodone is among the most commonly prescribed opioids for pain treatment. Studies have demonstrated marked variability in the pharmacokinetics (PK) of oxycodone which may be due to genetic variation. Although 80% of oxycodone breakdown occurs via cytochrome P450 3A4 into an inactive metabolite, up to 11% occurs through CYP2D6 into oxymorphone. Oxymorphone has 40 times the affinity and 8 times the potency of oxycodone upon Mu-opioid receptors. Therefore, the CYP2D6 ultra-rapid metabolizer genotype (UM) may confer risk for serious side effects with commonly prescribed doses. This suggests the need to rationalize oxycodone dosing regimens in pediatric population. Understanding oral oxycodone pharmacokinetics (PK) and pharmacogenomics (PG) favors the safe and effective use of this analgesic. The aim of this study is to characterize the effect of different CYP2D6 genotype on PK of oxycodone and its metabolites (oxymorphone, noroxymorphone and noroxycodone) in pediatric surgical patients.
Methods: This prospective cohort, single-center trial was approved by the hospital investigational review board. A total of 44 opioid-naive children, aged 0-5 years, scheduled for in-patient surgery, have been consented. A total of 11 Blood samples over 24 hour period were collected for the assay of oxycodone and its main metabolites, as well as for CYP3A4 and CYP2D6 genotyping. Plasma oxycodone, oxymorphone, noroxymorphone and noroxycodone levels were assayed using liquid chromatography- mass spectrometry (UPLC/MS/MS) and single-dose pharmacokinetics parameters were determined. CYP2D6 genotyping on the AffyMetrix DMET Plus panel augmented with three extra primers was used to identify ultra-rapid metabolizers.
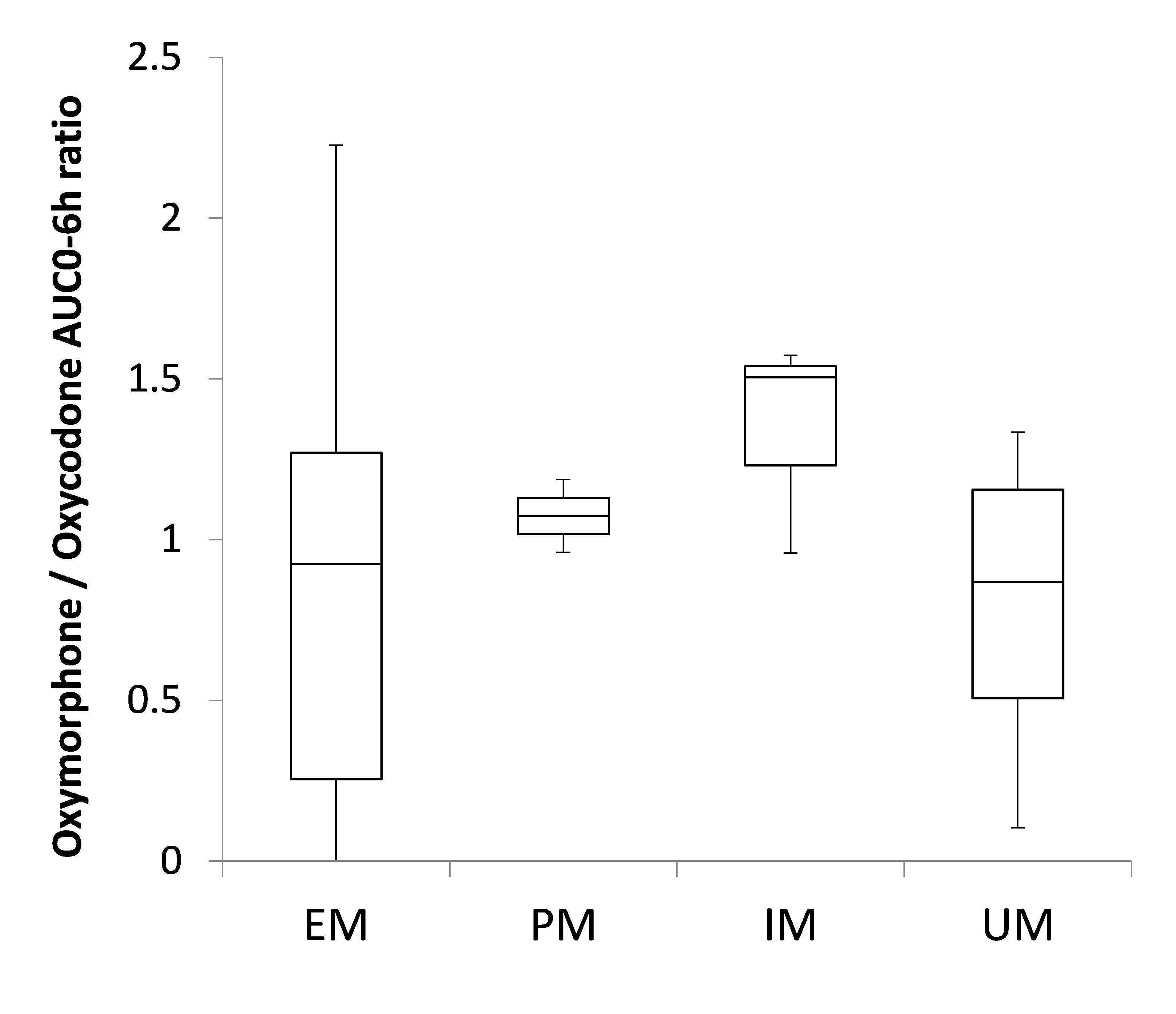
Results: All patients were wild-type normal metabolizers for CYP3A4, but there are significant differences in oxycodone plasma concentrations when analyzed in the context of the CYP2D6 phenotype. Mean (standard deviation) of area under the curve 0-6 hours (AUC 0-6h) of oxycodone were 24.28 (15.57), 27.86(40.72), 8.28(6.23), 36.29(18.4) in Extensive metabolizer (EM) group (n=33), Poor metabolizer (PM) group (n=3), Intermediate metabolizer (IM) group (n=3) and Ultra-rapid metabolize (UM) group (n=5) respectively. Median of AUC 0-6h of oxymorphone/oxycodone were 0.92, 1.07, 1.50, 0.87 in EM, PM, IM and UM group respectively.
Conclusion: Pharmacokinetics data revealed a substantial interpatient PK variability in pediatric surgical patient. We observed some differences in AUC 0-6h of oxycodone and ratio of AUC 0-6h for oxymorphone/oxycodone between CYP2D6 genotypes, although not all statistically significant yet, requiring further enrolment.
-
 PR1-161 Image 1
PR1-161 Image 1
Top










