
NM-338
A comparison of supraglottic devices in pediatric patients
1Syed F, 1Hakim M, 2Hakim M, 1Tumin D, 1Veneziano G, 1Tobias J, 1Krishna S
1Nationwide Children's Hospital, Columbus, OH, United states; 2Montefiore, Bronx, New york, United states
Introduction: When managing patients with a difficult airway, various supraglottic devices have been used as rescue airway devices. Our current study was aimed at comparing the fiberoptic view through the internal aspect of two different supraglottic devices, the i-gel® and the air-Q® LMA, in pediatric patients.
Methods: Patients ≤ 19 years of age, receiving a supraglottic airway as part of standard anesthetic care were enrolled and randomized to one of two types of supraglottic devices: i-gel® or air-Q® LMA. Following placement of the supraglottic device, a flexible fiberoptic bronchoscope was inserted through the stem of the supraglottic device to visualize the glottic aperture. The bronchoscopic view obtained was graded using the following scale: grade 1 = vocal cords seen completely; grade 2 = vocal cords and posterior epiglottis seen; grade 3 = vocal cords and anterior epiglottis seen; grade 4 = vocal cords not seen, but adequate ventilation occurs; grade 5 = vocal cords not seen, ventilation inadequate. A Fishers’ exact test and a contingency table were used to compare the fiberoptic view through the two different supraglottic devices. The percentage of acceptable or good views (grade 1 or 2) was compared to poor view (grade 4 or 5). Also noted were the time taken for insertion of each device, device size, number of attempts, technique of insertion, the ability to seal the airway at 20 cmH2O, and the time to achieve best view. Data are presented as mean ± SD.
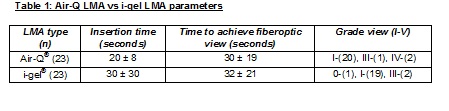
Results: Forty-six patients (23 in each group) have been enrolled to date, with ages ranging from 1 to19 years (mean: 11 ± 5) and weight ranging from 11 to 106 kg (mean: 50 ± 27). The size of the Air-Q® LMA varied from 1.5-4.5 and the size of the i-gel® device from 2-5. One patient in the i-gel® group was excluded from analysis due inadequate ventilation. In 1 case, the i-gel® supraglottic device was replaced with an Air-Q® LMA after completion of data collection due to loss of ventilation. In another patient, the Air-Q® LMA was replaced with an Ambu® LMA after study data were obtained due to problems with placement of the EGD scope. An acceptable view was attained in 20 of 23 cases in the Air-Q® group and 19 of 22 cases in the i-gel® group (p=NS). One patient in the i-gel® group and none in the Air-Q® group had inadequate ventilation when the best view was obtained. Insertion time did not significantly vary between the Air-Q® and i-gel® (20 ± 8 vs. 30 ± 30 seconds, p=0.111). Likewise, time to achieve fiberoptic view of the glottis through the device was similar between the 2 groups (30 ± 19 vs. 32 ± 21 seconds, p=0.730). Seven Air-Q® and 5 i-gel® supraglottic devices sealed the airway at 20 cmH2O.
Discussion: In terms of both the time required for successful placement and the rate of successful placement, the air-Q® LMA was similar to the i-gel® supraglottic device. Our data also shows no difference between the devices regarding glottic view.
-
 NM-338 Image 1
NM-338 Image 1
Top










