
NM-327
A comparison of intraoperative versus ICU blood utilization on outcomes in pediatric cardiac surgical patients.
Goswami D, Kenney M, Wadia R
Johns Hopkins Hospital, Baltimore, MD, USA
Introduction: Pediatric cardiac surgery patients account for a large portion of the blood utilization in a children’s hospital. The patients undergoing bypass get transfused frequently, and transfusion is an isolated risk factor for morbidity and mortality.1,2 There is little evidence on OR transfusion practices and effect on morbidity for congenital cardiac patients. The purpose of this study is to evaluate the morbidity and mortality risks in cardiac surgical patient based on volume transfused in cyanotic and acyanotic patients in the intensive care unit and operating room. Our hypothesis is that escalating OR transfusions will not have a direct correlation on morbidity and mortality while escalating ICU transfusions will. Our secondary hypothesis is that cyanotic patients will receive more transfusions in both the OR and the ICU than acyanotic patients.
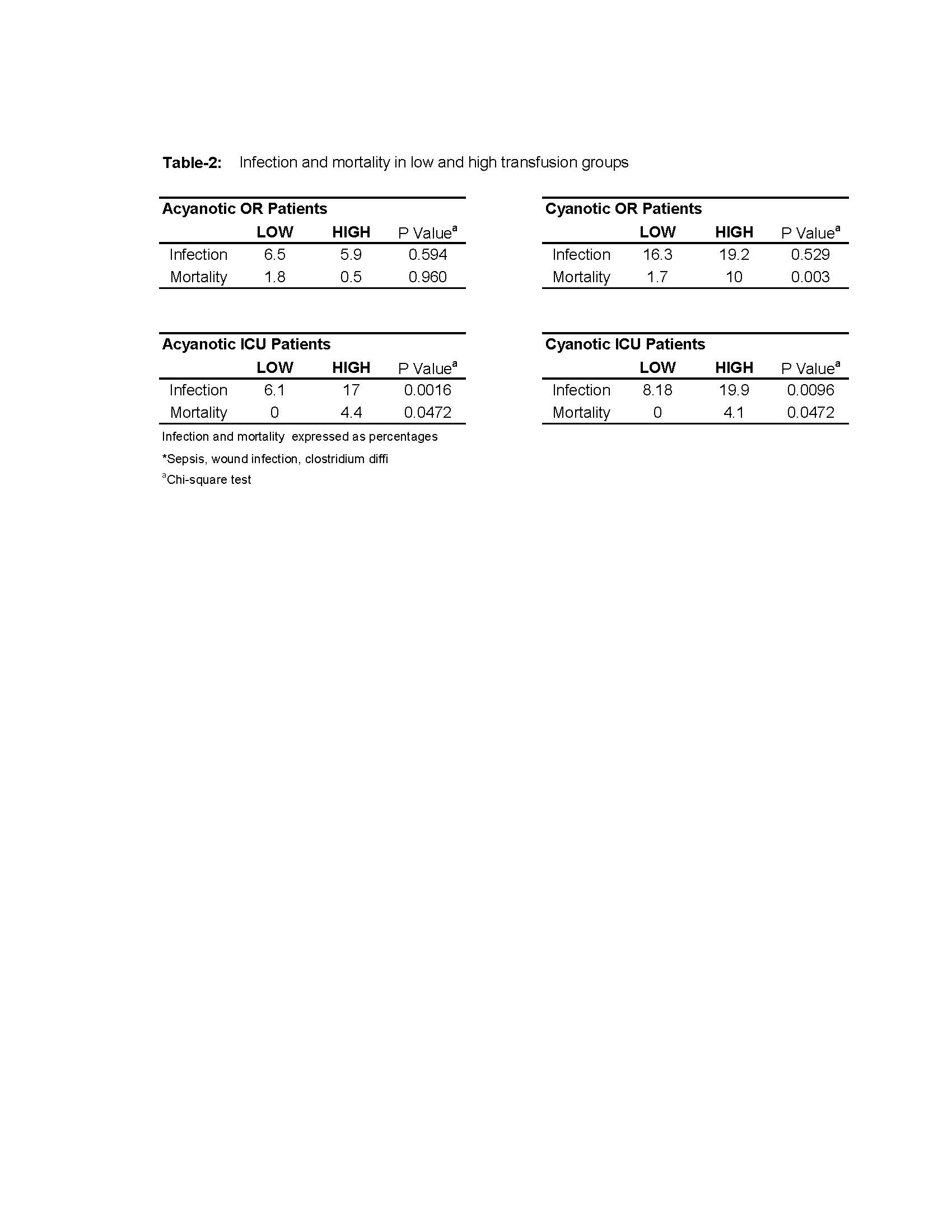
Methods: We reviewed our cardiac surgical cases from 2010-2017 using our previously reported STS and blood management and outcome database.3 The medians for transfused red cells were obtained for cyanotic and acyanotic patients in both the ICU and OR. Patients were excluded if they received no transfusion or transfused greater than the 95% percentile. These groups were then separated into low- and high-transfusion cohorts. The primary outcome measures were infection, mortality and length of stay. We completed our analysis using chi-squared test.
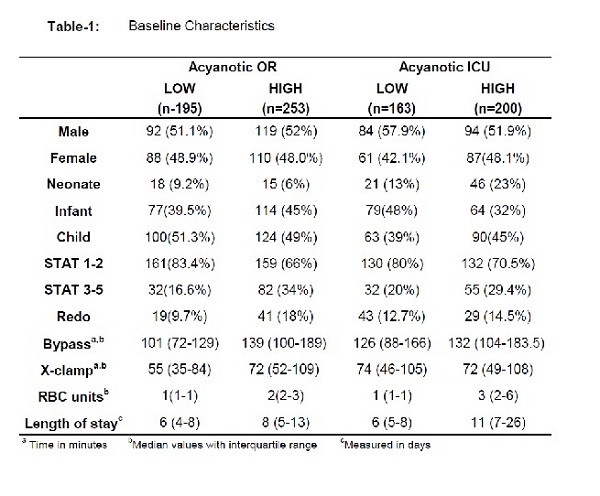
Results: Baseline demographic and clinical characteristics of each subgroup are described in Table-1. The rate of clinically suspected infection and mortality among the low versus high transfusion groups was statistically significant (p<0.05) in the ICU for both acyanotic and cyanotic patients (Table-2). The only statistically significant outcome in the OR was mortality in cyanotic patients.
Discussion: The results support our hypothesis that escalating transfusions do not have a similar effect in the OR when compared to the ICU. Cyanotic patients also received increased transfusions supporting our secondary hypothesis. Our study suggests that outcomes from OR transfusions may not be as simple as a direct association with the number of transfusions. This may be due to the filtration that occurs on bypass or the physiologic effects of transfusing for active hemorrhage rather than threshold hemoglobin level as in the ICU, among other possibilities. There were also differences seen in outcomes when comparing cyanotic and acyanotic patients.
Conclusion: Further studies are needed to isolate OR transfusion risk factors in acyanotic and cyanotic congenital heart disease.
1.Chambers Transfusion 1996 2. Lavoie Peds Anes 2011 3. Engorn SPA 2017
-
 NM-327 Image 2
NM-327 Image 2 -
 NM-327 Image 1
NM-327 Image 1
Top










