
OT-119
Asthma Can Cause Plastic Bronchitis?
Ma C, LeFevre A, Rosenberg E
Emory University, Atlanta, GA, USA
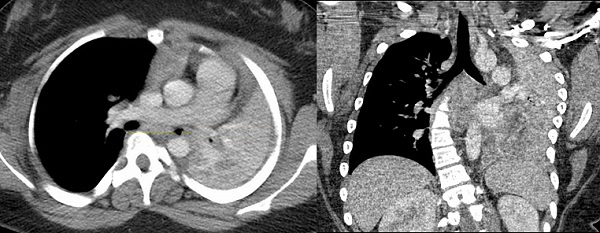
Plastic bronchitis (PB) is a rare disease of unclear etiology with a possible poor prognosis. Associations include congenital heart disease, asthma, toxic inhalation, sickle cell disease, pulmonary lymphatic abnormalities and influenza A. Mortality can reach 60% depending on the associated disease and cast type. Here, we describe the perioperative management of a patient with asthma and PB at our institution.
Our patient was a 12 year old obese female with poorly controlled asthma requiring 5 hospitalizations within the past year. She was transferred from an OSH to our PICU for management of status asthmaticus and pneumonia. Previously, flexible bronchoscopy demonstrated fibrinous inflammatory exudates with eosinophils and Charcot-Leydon crystals, consistent with PB. Prior to transfer she received magnesium, steroids, nebulizer treatments and terbutaline infusion without improvement. Chest physiotherapy, inhaled TPA, and azithromycin were initiated in the PICU, also without improvement.
On hospital day 5, she was taken to the OR for cast removal with rigid and flexible bronchoscopy. She had an uneventful IV induction of general anesthesia followed by tracheal intubation. Pulmonology was unsuccessful in cast removal with flexible bronchoscopy. She was then extubated by ENT for rigid bronchoscopy. During removal of a large, left bronchial mainstem cast, debris became lodged in the trachea and was unable to be removed or advanced. Our patient suffered near cardiopulmonary arrest due to poor ventilation and oxygenation and was emergently cannulated to V-V-A ECMO. Once on ECMO, ENT removed several more large casts, however many remained. Vascular surgery was consulted intraoperatively for left and right femoral arterial injuries sustained during ECMO cannulation.
Postoperatively, she underwent multiple bronchoscopies for cast removal while on ECMO in the PICU. She was decannulated from V-V ECMO on POD 7 and extubated on POD 24. Currently, she is followed closely in pulmonology clinic, remains on an aggressive airway clearance regimen and returns frequently to the OR for cast removal.
Plastic bronchitis is a rare, poorly understood disease characterized by potentially catastrophic airway obstruction. Prevention, supportive care and repetitive bronchoscopic cast removal are mainstays of management. There is a paucity of literature on the perioperative management of PB. Intervening on these patients at a facility with ECMO capabilities should be considered as rapid and profound clinical deterioration is possible. Further research is imperative to improve our understanding of the pathophysiology of PB and discovering new treatment options.
-
 OT-119 Image 2
OT-119 Image 2 -
 OT-119 Image 1
OT-119 Image 1
Top










