
CA-35
Validation of capnodynamic determination of cardiac output (Effective Pulmonary Blood Flow, COEPBF) during hypoxia induced pulmonary hypertension and inhaled nitric oxide treatment in piglets
1Karlsson J, 1Lonnqvist P, 2Wallin M, 2Hallbäck M
1 Karolinska University Hospital, Solna, Stockholm, Sweden; 2Maquet Critical Care AB, Solna, Stockholm, Sweden
Background: Pulmonary arterial hypertension (PHT) and hypoxia is associated with significant perioperative risk for major complications in children including pulmonary hypertensive crisis and cardiac arrest.
Capnodynamic assessment of CO has been validated in both smaller and larger animals with excellent agreement and trendability when compared with gold standard methods, e.g. Transonic Doppler CO (COTS) and Pulmonary Artery Cather Thermodilution (1-2).
We have in a previous study validated effective pulmonary blood flow (COEPBF) for its ability to measure non shunted pulmonary blood flow during normal, low and high CO in infants (results presented at moderated poster sessions SPA and CCAS 2017 Austin Texas).
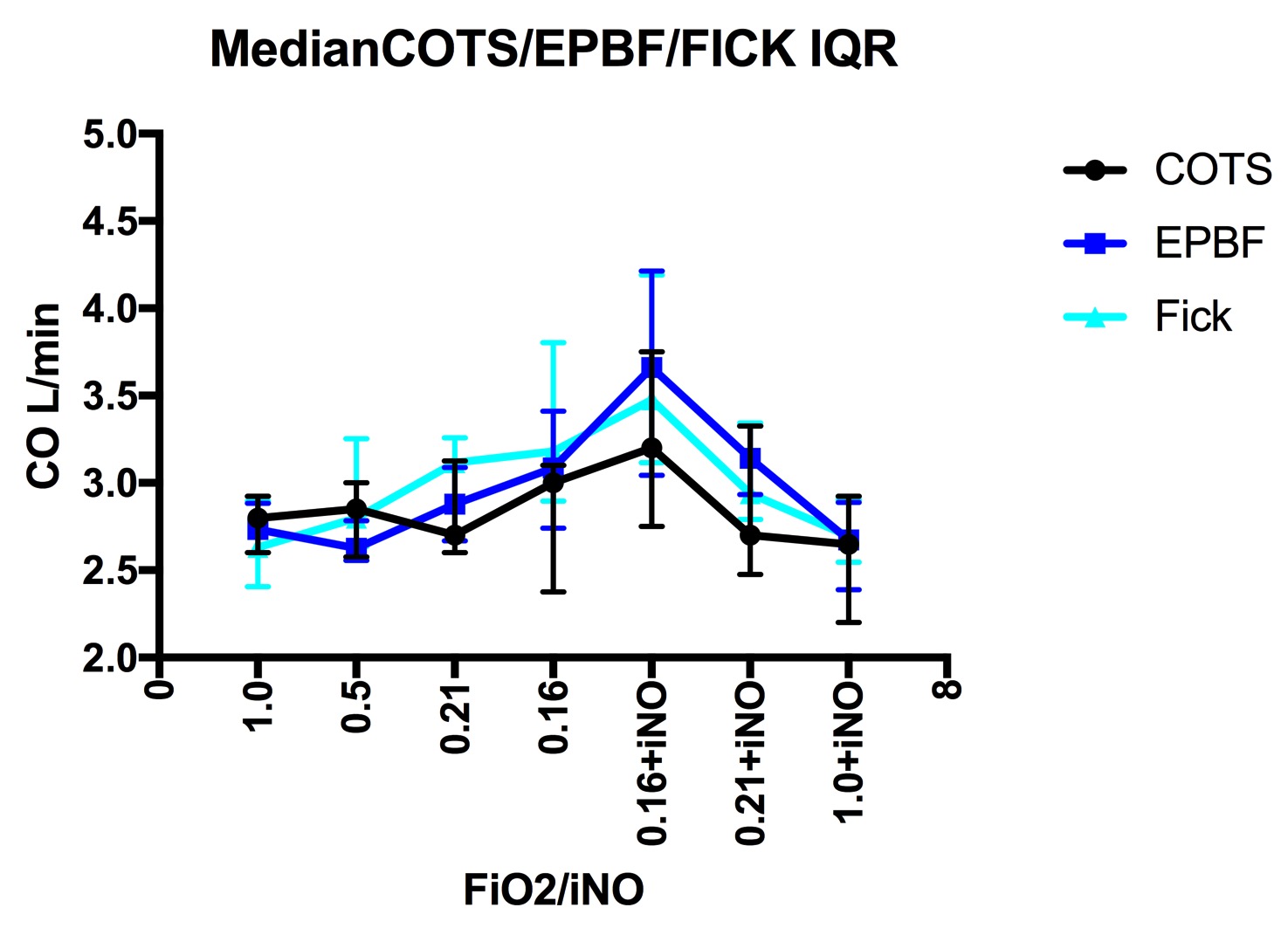
In the current study we have compared COEPBF with direct CO2 Fick (COFick) and COTS, during hypoxia induced selective acute pulmonary hypertension (PHT) and inhaled nitric oxide treatment in piglets.
Setting: Hedenstierna laboratory Uppsala Sweden
Method: 12 piglets were anaesthetized and mechanically ventilated and exposed to gradually declining FiO2 with the intent to increase pulmonary vascular resistance to a minimum of 200% from baseline. PHT was then reversed by adding 20 PPM inhaled nitric oxide. COEPBF, COFick and COTS were recorded simultaneously. Paired absolute values were compared using Bland-Altman analysis and trending ability was assessed using concordance analysis.
Results : All animals showed a desirable increase in PVR during hypoxia and strong attenuation of PHT after inhalation of 20 PPM nitric oxide. COEPBF showed an agreement with COTS of -0,25 L/min (limits of agreement -1 and +0,5 L/min) with a mean percentage error of 25%. COEPBF and COFick had an agreement of -0,08 L/min (limits of agreement -0,8 and +0,7 L/min) and a mean percentage error of 24%. COTS and COFick had an agreement of -0,25 L/min (limits of agreement -1 and +0,5 L/min) and a mean percentage error of 28% The concordance rate was 94% for COEPBF when compared with COTS using 10% exclusion zone.
Conclusion: Estimation of CO and pulmonary blood flow using COEPBF is interchangeable with the reference methods (gold standards) COFick and COTS. This suggests that COEPBF is an accurate and valuable tool for monitoring pulmonary blood flow and cardiac output in pulmonary hypertension and during hypoxia. COEPBF could also be an important tool in guidance of inhaled nitric oxide treatment of PHT.
References
1. 1. Hällsjö Sander et al. Novel continuous capnodynamic method for cardiac output assessment during mechanical ventilation. Br J Anaesth. 2014 May;112(5):824-31.
2. Sander CH et al. A modified breathing pattern improves the performance of a continuous capnodynamic method for estimation of effective pulmonary blood flow. J Clin Monit Comput. 2017 Aug;31(4):717-725
-
 CA-35 Image 1
CA-35 Image 1
Top










