
GA3-72
Adrenal suppression from prenisolone ophthalmic drops in a 5-week-old male
Fast J, Volz L
University of Wisconsin, Madison, WI, USA
Introduction:
Glucocorticoids were initially prescribed to treat rheumatoid arthritis in 1939, but today their uses range from asthma to skin disorders, and come in myriad formulations. Long-term use is associated with side effects including the classic “buffalo humpâ€, impaired glucose control, growth suppression in children, and adrenal dysfunction that leads to suppression of endogenous cortisol production. The following case describes intraoperative hypotension secondary to adrenal suppression in an infant exposed to long-term prednisolone eye drops.
Case Presentation:
A five-week-old term infant with congenital glaucoma presented for outpatient repeat trabeculotomy. Genetic karyotyping and neonatal metabolic screening were normal. He underwent an uncomplicated trabeculotomy under general anesthesia 21 days ago, and has been taking 1% prednisolone eye drops since then. He now weighs 4.4 kilograms and is 46 weeks post menstrual age.
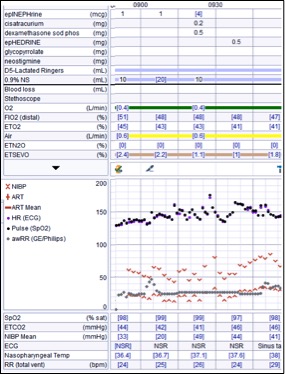
Inhalation induction, peripheral IV placement, administration of propofol 2 mg/kg, and intubation were uncomplicated. Initial mean arterial pressure (MAP) via noninvasive blood pressure (NIBP) monitor was 25 mmHg, increasing to 34 on second check. No opioids were administered. Intraoperative intravenous fluids totaled 150 mL. After incision, the patient’s MAP again fell and ST segment depression was noted on ECG. Attempts to increase MAP by decreasing volatile gas and administering fluid boluses and small boluses of epinephrine were unsuccessful. We then considered adrenal suppression from prednisolone exposure. A dose of dexamethasone was given, after which time the MAP increased and ST segments normalized. The remainder of the case was unremarkable, extubation was uncomplicated, and the patient was discharged home later in the afternoon.
Discussion:
Adrenal suppression is most commonly iatrogenic as a result of corticosteroid administration, and relatively small doses can lead to suppression. We estimated a daily dose of 0.45 mg/kg of prednisolone for this patient, if administered appropriately (1% prednisolone [10mg/ml x 4 drops/day x ~0.05 mL/drop] x ~4 kg patient weight). The exact dose cannot be quantified due to variables including: drop volume variability, systemic uptake in the patient, drug pharmacokinetics, and proper adherence to the prescription. This case is an interesting and reinforcing example of the power of exogenous steroid use, even through a vehicle as seemingly benign as eye drops.
1. Chrousos, Pavlaki AN, Magiakou MA. Glucocorticoid Therapy and Adrenal Suppression. [Updated 2011 Jan 11]. In: De Groot LJ, Chrousos G, Dungan K, et al. (eds). Endotext. South Dartmouth (MA): MDText.com, Inc.; 2000-. https://www.ncbi.nlm.nih.gov/books/NBK279156/
2. German EJ, Hurst MA, Wood D. Reliability of drop size from multi-dose eye drop bottles: is it cause for concern? Eye (Lond). 1999;13 ( Pt 1):93-100.
-
 GA3-72 Image 1
GA3-72 Image 1
Top










