
NM-219
Anesthetic Management for Clamshell Thoracotomy: Resection of a Fetiform Teratoma Occupying the Entire Hemithorax Leading to Airway and Cardiac Compression
Abhold E, Chang A
Massachusetts General Hospital, Boston, Massachuse, United states
Teratomas are a rare type of germ-cell tumors often comprised of multiple tissue types. Mediastinal teratomas are a rare presentation of teratomas associated with the same risks as other mediastinal masses. These risks include airway and hemodynamic compromise due to mass effect which pose significant anesthetic risks. In this case report, we share our experience in anesthetic management for clamshell thoracotomy resection of a large fetiform teratoma occupying the entire hemithorax in a previously healthy 3-year old boy.
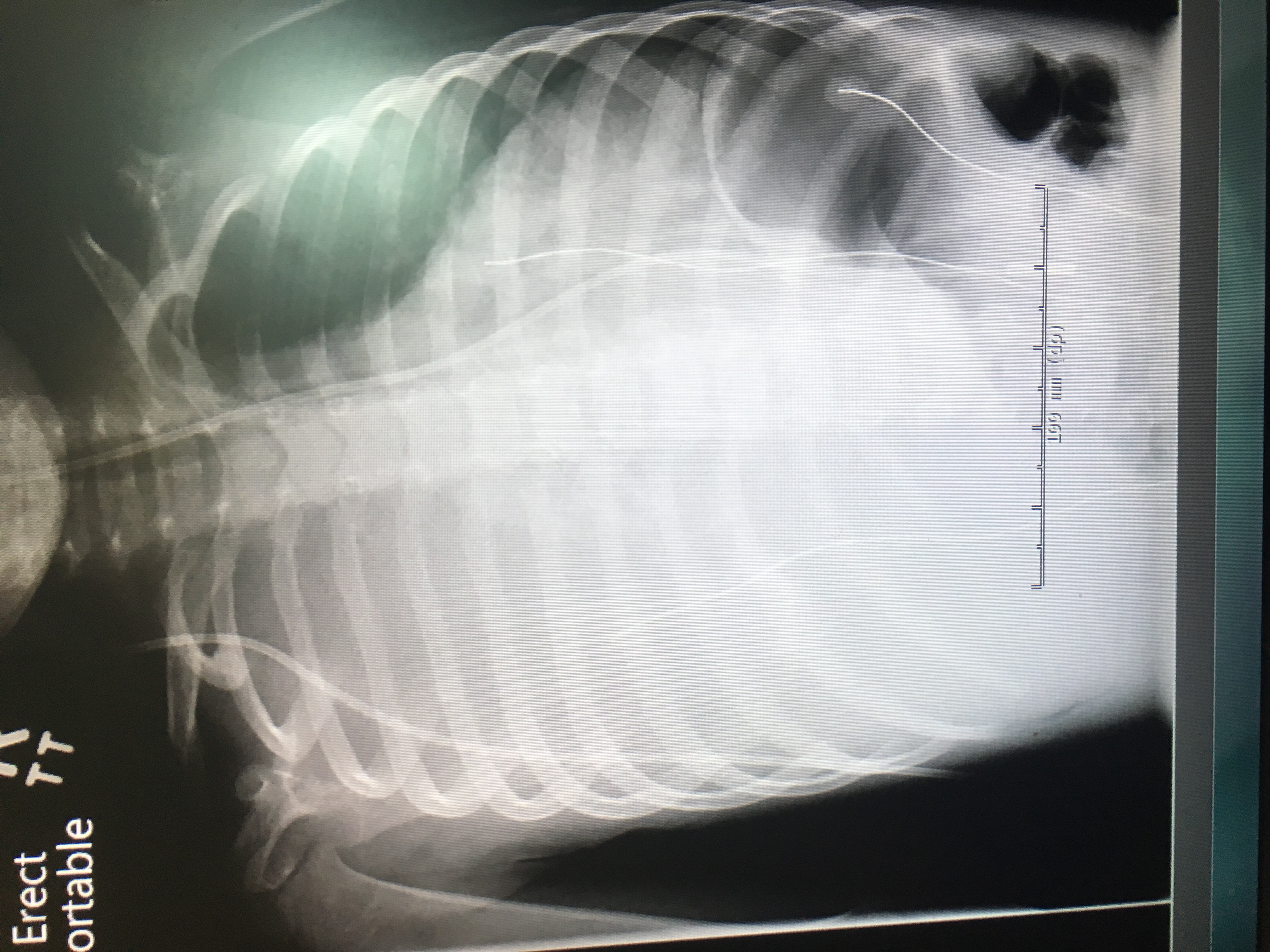
Our patient initially presented with progressive shortness of breath and decreased activity level over 3 months. His mother noted that he increasingly laid on his right side for sleep and to ease his work of breathing. On exam, he had complete absence of breath sounds in the right chest along with distant heart sounds. Chest x-ray demonstrated complete occupation of the right hemithorax by a heterogeneous mass with mediastinal shift to the left (Figure 1). A CT chest/abdomen with contrast demonstrated a mass with several tissue densities completely filling the entire right hemithorax causing significant tracheal compression above the level of the carina and complete occlusion of the right main bronchus. The heart was displaced completely into the left hemithorax with compression of the great vessels and the right atrium (Figure 2).
The surgical plan was clamshell thoracotomy for evacuation of mass by cardiac surgery. Due to the concern for airway and hemodynamic collapse on induction, rigid bronchoscopy, ENT surgery, and cardiac surgery with ECMO equipment were on standby during induction of anesthesia. Pre-induction IV access was present and the induction proceeded with mask induction maintaining spontaneous ventilation. The patient was deepened on sevoflurane and intubated without complications. Additional large bore IV access and an arterial-line were obtained post-induction. There was discussion regarding thoracic epidural placement for post-operative pain management, but due to potential need for intraoperative heparinization for cardiopulmonary bypass (CPB), we did not place an epidural initially. Surgical resection proceeded via clamshell thoracotomy and a mass measuring 20 cm x 15 cm was removed from the thoracic cavity without the need for CPB. The patient required intraoperative transfusions and remained hemodynamically stable. The patient was brought intubated postoperatively to the ICU, and a thoracic epidural was placed at the bedside in the ICU. The mass was determined to be a fetiform teratoma of mediastinal origin on pathology with many tissue elements including renal, hepatic, gastrointestinal and vertebral elements (Figure 3).
As a part of this presentation, we plan to review the differences between mature/immature teratomas, fetiform teratomas, and fetus in fetu. We also plan to review the key radiographic features of a mediastinal mass with hemodynamic consequences.
-
 NM-219 Image 1
NM-219 Image 1
Top










