GA4-91
An unknown diagnosis and a series of unfortunate events leading to an infant’s demise
Pukish J, Reddy S
Children's National Medical Center, Washington, DC, USA
INTRODUCTION
Effective communication is a central skill necessary for all health care providers, particularly during life threatening patient events. While the role of clear, decisive communication has been well established, the role of communication in formulating appropriate patient management strategies has been thoroughly examined. We present the tragic case of a patient that highlights the sad reality that medical error vulnerability is increased when healthcare team members are under stress or in high-task situations.
CASE PRESENTATION
A 4-month old 3.26 kg infant with mild hypotonia & failure to thrive, born full term via emergent c-section due to intrauterine growth restriction & oligohydramnios presented to outpatient neurology clinic for workup for her hypotonia. On exam, she was found to have increased work of breathing & cyanosis while crying. She was transferred to the ED & eventually to the PICU for deteriorating respiratory status.
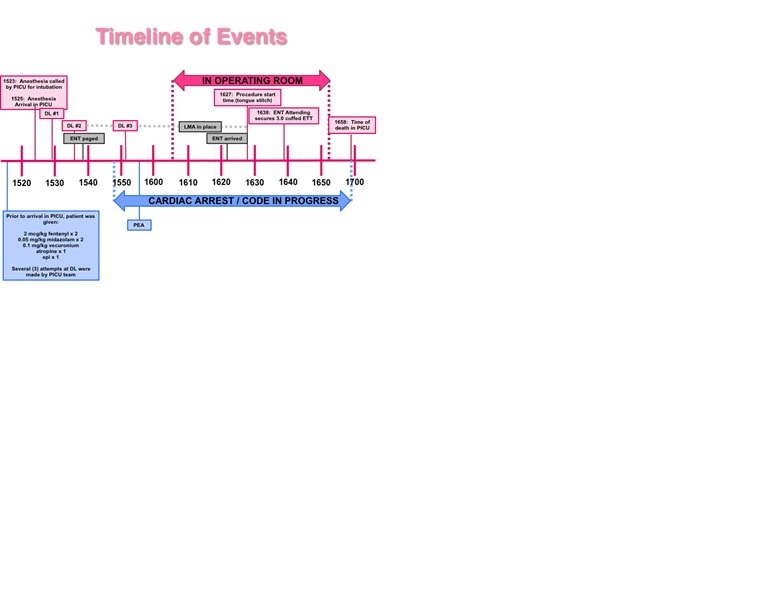
Eighteen hours later, despite RAM Cannula & several doses of albuterol,the patient continued to demonstrate signs of impending respiratory failure. The PICU team made the decision to intubate, but after three failed attempts, called the anesthesia team for assistance. After two intubation attempts by the anesthesiologist, ENT was paged, however, the patient went into cardiac arrest & resuscitation was initiated, including placement of LMA during transit to the OR. During this period, the infant’s abdomen became tense & would not decompress despite numerous attempts at suctioning the stomach. Resuscitation continued in the OR, ENT attending placed a tongue stitch & 11 minutes later, secured a 3.0 cuffed ETT. The patient was transferred back to the PICU where she was pronounced dead.
DISCUSSION
An autopsy determined the cause of death to be severe laryngeal stenosis complicated by abrupt respiratory compromise associated with symptoms of an upper respiratory infection. Examination of respiratory tract revealed an anteriorly displaced larynx with edematous epiglottis & arytenoids, congenital laryngeal stenosis (2.0 mm), normally formed lungs with pulmonary edema &hemorrhage. Musculoskeletal survey revealed a short sternum, overlapping 2nd & 4th fingers & a prominent palmar crease, consistent with postmortem genetic testing of 22q deletion syndrome. While the patient clearly had airway anomalies that were the ultimate cause of her demise, there were several management opportunities that could have occurred during this tragic event that might have altered the outcome:
• 18 hours lapsed from the time of admission to decision to intubate. Should an elective intubation have been performed earlier?
• Should muscle relaxant have been avoided? Should initial attempt at airway have been made by a PICU attending or an anesthesiologist instead?
• Should a surgical airway or expanded airway management have been performed at bedside by ENT instead of going to the OR?
-
 GA4-91 Image 1
GA4-91 Image 1
Top