
NM-220
Routine preoperative laboratory testing in elective pediatric cardiothoracic surgery patients: a survey of current practices
1Jones S, 1Jooste E, 2Gottlieb E, 3Schwartz J, 3Goswami D, 4Gautam N, 5Benkwitz C, 6Downey L, 6Guzzetta N, 7Zabala L, 8Latham G, 9Navaratnam M, 9Wise-Faberowski L, 10McDaniel M, 11Spurrier E, 1Machovec K, 12Faraoni D
1Duke University Medical Center, Durham, North caro, United states of america; 2Texas Children's Hospital, Baylor College of Medicine, Houston, Texas, United states of america; 3Johns Hopkins Children's Center, Baltimore, Maryland, United states of america; 4The University of Texas Medical Center at Houston, Houston, Texas, United states of america; 5University of California at San Francisco School of Medicine, San Francisco, California, United states of america; 6Emory University School of Medicine, Children's Healthcare of Atlanta, Atlanta, Georgia, United states of america; 7University of Texas Southwestern Medical Center, Dallas, Texas, United states of america; 8Seattle Children's Hospital, Seattle, Washington, United states of america; 9Lucile Packard Children's Hospital, Stanford University, Palo Alto, California, United states of america; 10University of North Carolina, Chapel Hill, North caro, United states; 11Nemours/Alfred I duPont Hospital for Children, Wilmington, Delaware, United states of america; 12The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada
Introduction
Preoperative laboratory testing for outpatient pediatric patients presenting for cardiac surgery is standard of care at most institutions. Laboratory evaluations are purportedly used to determine patient fitness for surgery and identify concerns that may need to be addressed prior to a procedure. However, recent studies examining the utility of preoperative lab testing found that routine testing is expensive for patients and hospitals and procedures are rarely cancelled due to laboratory abnormalities.1 We conducted a survey of pediatric cardiac anesthesiologists to define current practices in preoperative laboratory testing and the perceived necessity for these studies prior to elective pediatric cardiothoracic surgery.
Methods
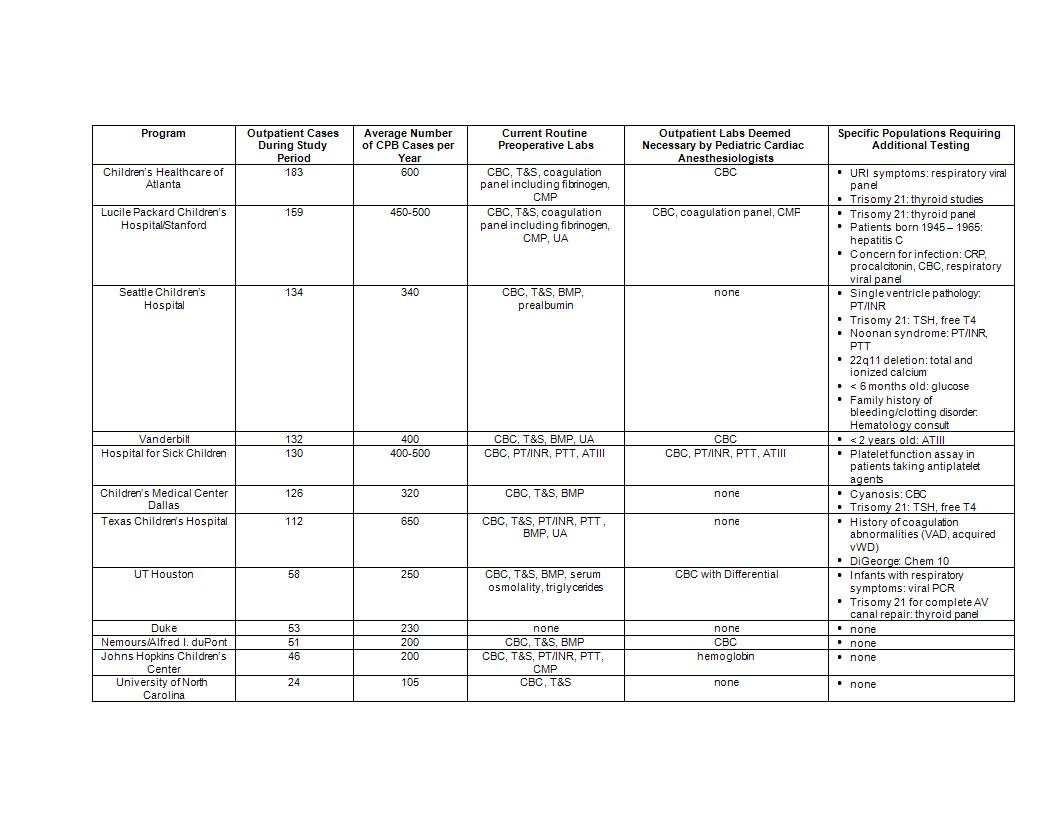
We surveyed pediatric cardiac anesthesiologists who are members of the Hemostasis Interest Group (HIG) within the Congenital Cardiac Anesthesia Society. Participating programs (n = 12) monitored their respective preoperative laboratory practice for six months, from 1 April 2017 to 30 September 2017, on pediatric outpatients presenting for pediatric cardiac surgery requiring cardiopulmonary bypass (CPB). Each institution assessed routine laboratory practices, laboratory tests deemed necessary by pediatric cardiac anesthesiologists, and which tests are reserved for specific patient populations. We assumed that all patients would receive a type and screen (T&S) and arterial blood gas (ABG) with hemoglobin prior to CPB initiation. Lastly, all programs were asked whether the availability of a particular routine laboratory value would have changed management if known prior to CPB.
Results
All institutions except one currently obtain routine preoperative laboratory studies (Table 1). Complete blood count (CBC) is considered necessary by the majority of institutions, while the need for metabolic panels and coagulation studies is more variable. Special populations requiring additional routine testing include those with trisomy 21, cyanotic congenital heart disease, patients taking anti-platelet agents, and patients who may be pregnant. Five institutions recommend fewer studies than is their current practice. No one reported an incidence where a particular data point would have changed management if known prior to CPB.
Discussion
Results of this survey display the variability in preoperative laboratory testing of outpatients presenting for pediatric cardiac surgery requiring CPB. These results should prompt further discussion as to which laboratory studies are necessary for safe management of elective pediatric cardiac surgery patients. Future studies should focus on the effects of minimizing preoperative testing to decrease hospital charges and patient cost while maintaining safe care.
References
1. Nieto RM et al. J Thorac Cardiovasc Surg. 2017;153:678-85.
-
 NM-220 Image 1
NM-220 Image 1
Top










