
PR2-174
Ultrasound guided transversalis fascia plane block for alveolar cleft repair with iliac crest bone graft
Ruby J, Kraemer F, Taylor J, Jackson O, Muhly W
Children's Hospital of Philadelphia, Philadelphia, PA, United states
Introduction: Alveolar cleft repairs are often completed with iliac crest bone graft (ICBG). ICBG harvesting is associated with patient morbidity including persistent pain at donor site, difficulty with ambulation, and limitations in daily activities.1 The transversalis fascia plane (TFP) block has been shown to be an effective technique for managing pain after ICBG harvesting in adults.2 We report the use of TFP block as an analgesic adjuvant in a series of pediatric patients undergoing alveolar cleft repair with autologous ICBG.
Methods: We identified and consented four patients undergoing alveolar cleft repair with ICBG for general anesthesia and a single shot TFP block. Following induction of general anesthesia, patients were positioned supine with a bump under the right hip. A linear ultrasound (US) probe was placed in the transverse orientation just superior to the iliac crest. The transversus abdominis (TA) and internal oblique muscles were traced posteriorly until they tapered into a common aponerousis. Using a 2†spinal needle, 0.5-1cc/kg of 0.2% ropivicaine was injected in the plane between the TA muscle and the underlying transversalis fascia. Anesthesia was maintained with sevoflurane and a standardized regimen of IV acetaminophen, ketorolac, and morphine titrated to effect. All patients were extubated and transported to the PACU. Postoperative pain scores, location of pain (when available), and opioid requirements were collected and reported.
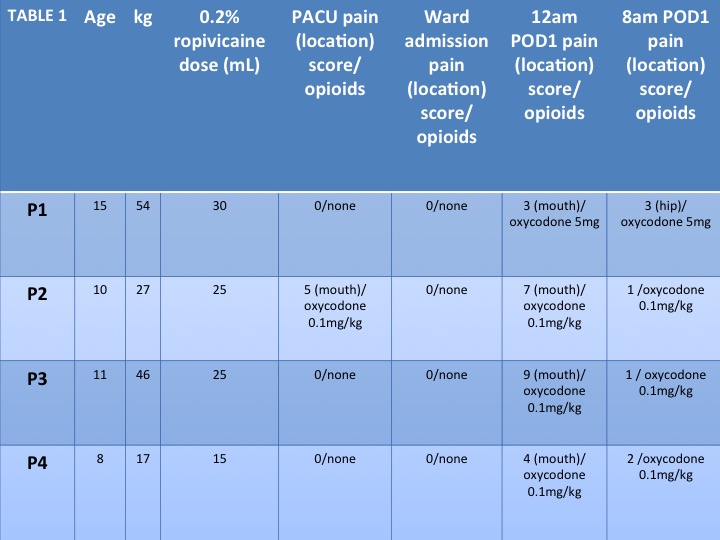
Results: Patient characteristics, pain scores and opioids given in the postoperative period are reported in Table 1. In addition to the TFP block and multimodal analgesics, patients received 0.1mg–0.15mg/kg of morphine intraoperatively. No patients required an IV opioid rescue dose in the PACU or postoperatively. No patients reported pain at the harvest site in the PACU. On the floor, patients received PRN oxycodone at a frequency of q4hr–q6hr. In all patients, the first site of pain documented was the mouth. Hip pain was only reported in one patient, which was 24 hours postoperatively. There were no adverse events or complications from the TFP block.
Discussion: Our small case series illustrates that an US guided TFP block is a potentially safe and efficacious strategy for multimodal pain management and decreasing opioids needed in pediatric patients undergoing alveolar cleft repair with ICBG. Further work is needed to determine the role of this block in the management of this patient population.
Conclusion: US guided TFP block may be a useful adjuvant in managing patients undergoing alveolar cleft repair with ICBG.
References
1. Morbidity at the Iliac Crest Donor Site following Bone Grafting of the Cleft Alveolus. Swan, M. British J of Oral and Maxillofac Surg. 2006. Vol 44: 129-133. 

2. US-guided Transversalis Fascia Plane Block Provides Analgesia for Anterior Iliac Crest Bone Graft Harvesting. Chin, K., et al. Can J Anes. 2012. 59: 122-123. 

-
 PR2-174 Image 1
PR2-174 Image 1
Top










