
GA1-54
Non triggering anesthetic management in a patient with Mastocytosis & von Willebrand Disease
Oosthuysen R, Nguyen T
Vanderbilt University Medical Center, Nashville, TN, United states of america
Mastocytosis is a rare condition with elevated levels of cutaneous and systemic levels of mast cells1. Increased levels of mast cells place patients at elevated risk for anaphylaxis from drugs and physical stimuli compared to the general population. Lifetime prevalence of anaphylaxis is up to 50% in adults. Anesthesia, particularly general anesthesia for major surgery, has been associated with increased risk of anaphylaxis - up to 6% of patients, noting some anesthetic agents have increased risk of histamine release2,3.
5 year old male with history of mastocytosis, craniosynostosis, obstructive sleep apnea and presumed von Willebrand disease (vWD) who presented for major cranial vault reconstruction.
The challenge:
Delivering an anesthetic that would mitigate any systemic mast cell degranulation which could lead to anaphylaxis and coagulopathy due to heparin release.
Treatment plan:
An IV attempted preoperatively to administer Factor VIII to treat coagulopathy due to chronic activation of mast cells.This failed due to patient being a difficult IV placement and agitation, proceeded to OR for inhalational induction.
Patient induced with standard ASA monitors, radial arterial line and two PIVs inserted.
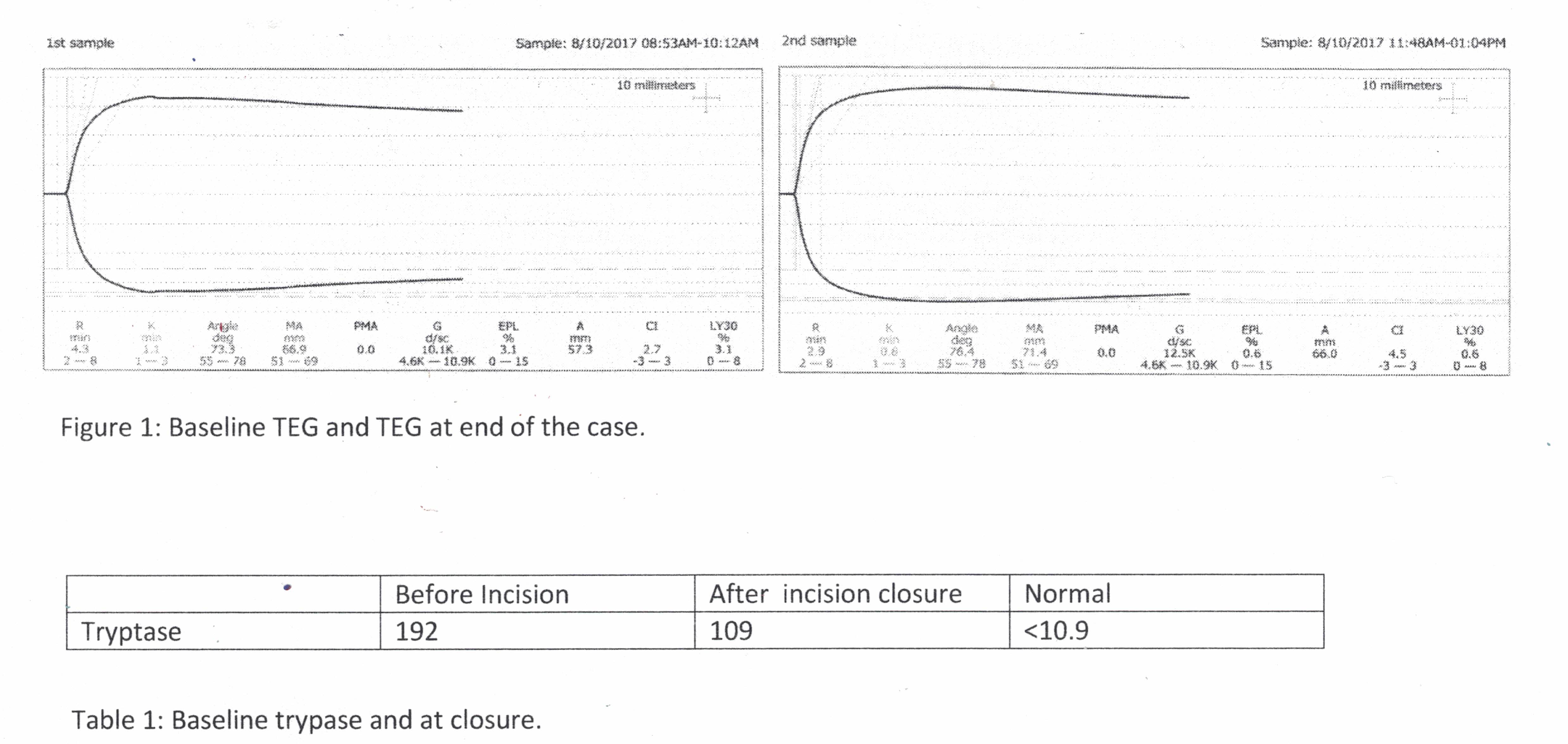
Baseline TEG and tryptase level obtained and then Factor VIII given for vWD
Methylprednisolone, diphenhydramine given for anaphylaxis prophylaxis.
Anesthesia maintenance consisted of drugs that did not increase histamine release. Isoflurane, vecuronium, fentanyl and aminocaproic acid infusion.
Patient hemodynamically stable throughout, TEG and tryptase levels repeated to look for signs of systemic mast cell degranulation (see figures).
Patient extubated and went to PACU then ICU uneventfully.
Discussion:
We were able to safely administer general anesthesia to this complex patient without major bleeding or triggering anaphylaxis. This was done by administration of appropriate hemostatic factors, prophylactic medications and avoiding histamine inducing anesthetic agents. Pre and post surgical tryptase levels support this. However, the abnormally high tryptase levels especially at the start of the case, 192, gives concern that physical stimuli such as attempting placement of PIV can lead to significant levels of histamine release in this patient population raising concern for physical stimulation induced anaphylaxis. While we avoided premedication in this case due to sleep apnea concerns, it should be given additional consideration in this population.
Works cited:
1. Muller, U.R., et al. The Problem of Anaphylaxis and Mastocytosis. Current Allergy and Asthma Reports. 2009, 9:64-70
2. Hermans, M et al. Management around invasive procedures in mastocytosis An update. Ann Allergy Asthma Immunology. 2017 Aug 30. pii: S1081-1206
3. Brockow, K. Anaphylaxis in Patients with Mastocytosis – A Prospective Study on Prevalence, Severity and Trigger Factors in 121 Patients. J Allergy Clinical Immunology Vol 117, Number 2, S307
-
 GA1-54 Image 1
GA1-54 Image 1
Top










