
OS1-137
Adenosine triphosphate monitoring of operating room surfaces
Ramirez A, Tumin D, Tobias J, Mohan S, Uffman J
Nationwide Children's Hospital, Columbus, Ohio, United states
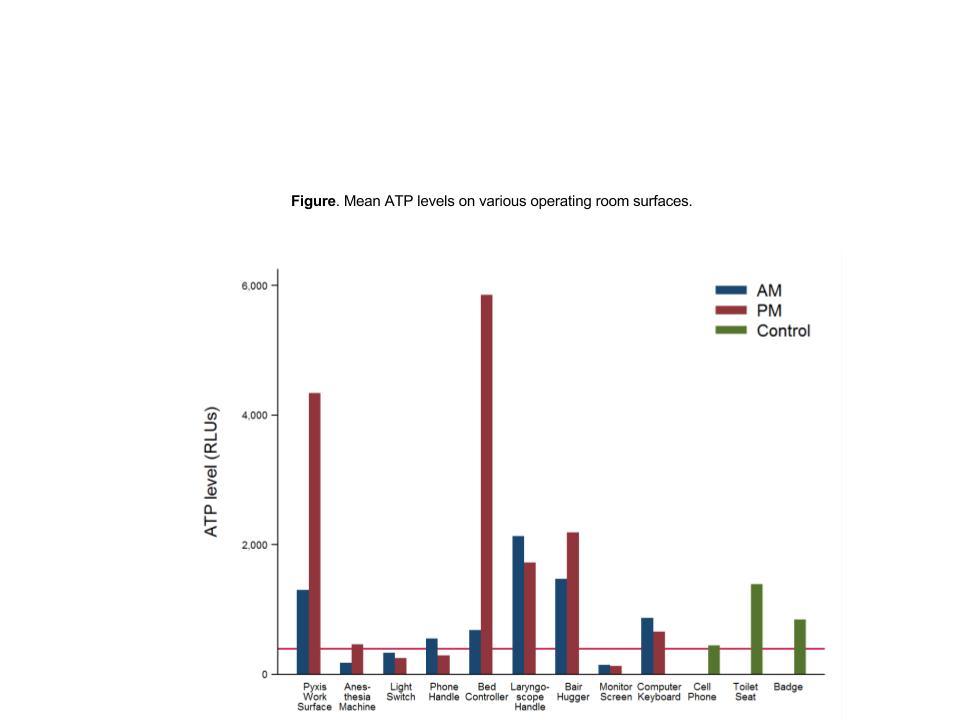
Introduction: Adenosine triphosphate (ATP) is an organic compound present on living organisms and serves as a surrogate for microbial contamination. Inadvertent contamination of the operating room (OR) setting may increase the risk of infection during surgical procedures. At our institution, we have used ATP monitoring to confirm environmental contamination in the intensive care unit, and to improve the effectiveness of cleaning practices. In the OR setting, we measured contamination of high-contact surfaces. We hypothesized that contamination would increase from morning (AM) to afternoon (PM), despite cleaning between cases. Secondarily, we compared the degree of OR contamination to various control sites.
Methods: ORs with high case turnover were selected for the study. Ten sites in each OR, selected based on likelihood of high staff contact, were swabbed using the AccuPoint® HC ATP Sanitation Monitoring device. This device measures the amount of ATP on a given surface and provides a numerical measure of contamination (relative light units or RLUs). Based on manufacturer standards, a surface was considered clean at ≤ 400 RLUs. AM measurements were taken prior to the start of surgical cases and PM measurements were taken on the same day after cases were completed. Control sites included samples of hospital toilet seats, staff cell phones, and staff hospital badges.
Results: A total of 80 morning and 70 afternoon samples were obtained from 8 ORs over 2 weeks. The highest average contamination level was found on OR floors (AM: 5800 ± 7109 RLUs; PM: 24,229 ± 34,897 RLUs). Average contamination of other sites is summarized in the Figure. No OR sites showed statistically significant increase in contamination from AM to PM. Among OR sites other than the floor, laryngoscope handles had the highest level of contamination in the AM (2,136 ± 2,862 RLUs), with 75% of AM samples and 100% of PM samples showing ≥ 400 RLUs. This level of contamination was comparable to data from hospital toilet seats (95% CI of difference: -957, 1733 RLUs; p=0.435; 90% of samples exceeding 400 RLUs). Results were consistent when examining median contamination levels.
Discussion: Apart from OR floors, laryngoscope handles emerged as a key site where improved cleaning practices at the beginning of the day may reduce infection risk. Our results did not show statistically significant differences in contamination between the AM and PM samples, offering tentative evidence that current cleaning practices during case turnover are effective. Continuation of this study will determine the utility of ATP monitoring for guiding infection control in the OR.
References:
1. Messina G, et al. Effectiveness of ATP bioluminescence to assess hospital cleaning: a review 2017;58:E177-83.
2. Amodio E, Dino C. Use of ATP bioluminescence for assessing the cleanliness of hospital surfaces: A review of the published literature (1990–2012). J Infect Public Health 2014;7:92-8.
-
 OS1-137 Image 1
OS1-137 Image 1
Top










