
OS2-149
Perioperative Outcomes and Management in LeFort III Midface Advancement Surgery: A Multicenter Study from the Pediatric Craniofacial Collaborative Group
1Glover C, 2Fernandez A, 3Huang H, 4Binstock W, 5Zhong J, 6Reid R, 7Dalesio N, 5Derderian C, 8Stricker P
1Texas Children's Hospital / Baylor College of Medicine, Houston, TX, USA; 2Johns Hopkins All Children’s Hospital, St Petersburg, FL, USA; 3Baylor College of Medicine, Houston, TX, USA; 4University of Chicago, Chicago, IL, USA; 5UT Southwestern, Dallas, TX, USA; 6University of Chicago Medicine, Chicago, il, USA; 7Johns Hopkins, Baltimore, MD, USA; 8The Children's Hospital of Philadelphia, Philadelphia, PA, USA
The Pediatric Craniofacial Collaborative Group established the Pediatric Craniofacial Surgery Perioperative Registry (PSCPR) as an international registry to evaluate practice patterns in children undergoing complex cranial reconstruction in an effort to improve perioperative quality and safety. The aim of this study was to utilize the registry in an effort to assess and compare management, outcomes, and complications in children undergoing LeFort III and Monobloc midface advancement procedures.
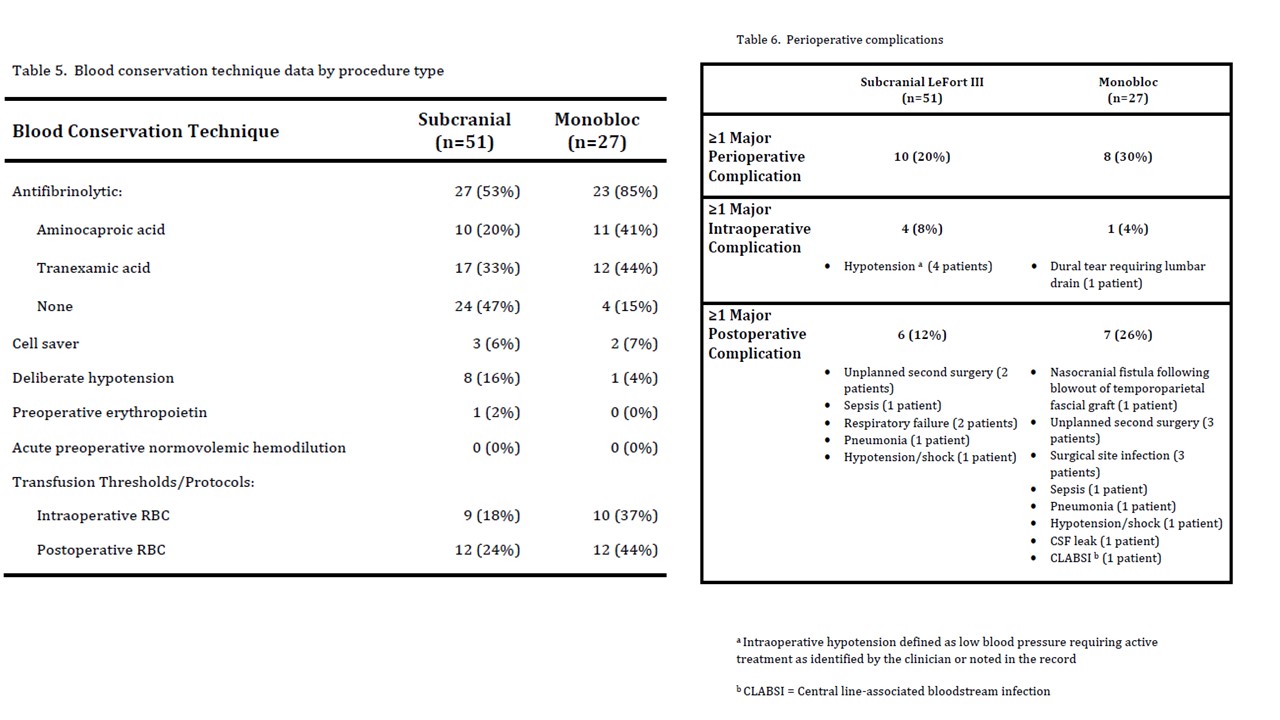
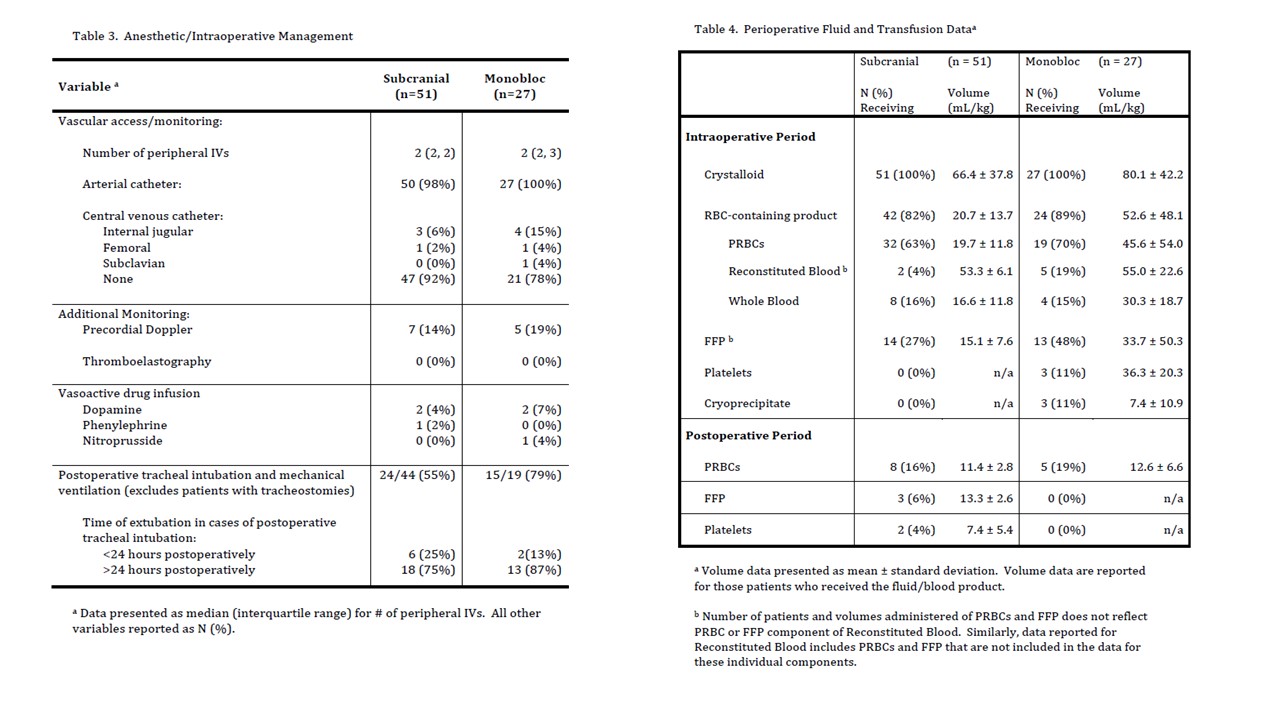
This observational, multi-institutional study included 20 centers who contributed data from June 2012 to September 2016. The database was queried for cases of LeFort III and Monobloc surgery. Data extracted included patient demographics, antifibrinolytic usage, fluid management, hospital length of stay, and blood conservation techniques. Outcomes included intraoperative and perioperative transfusion volumes, total blood donor exposures, and length of hospital stay.
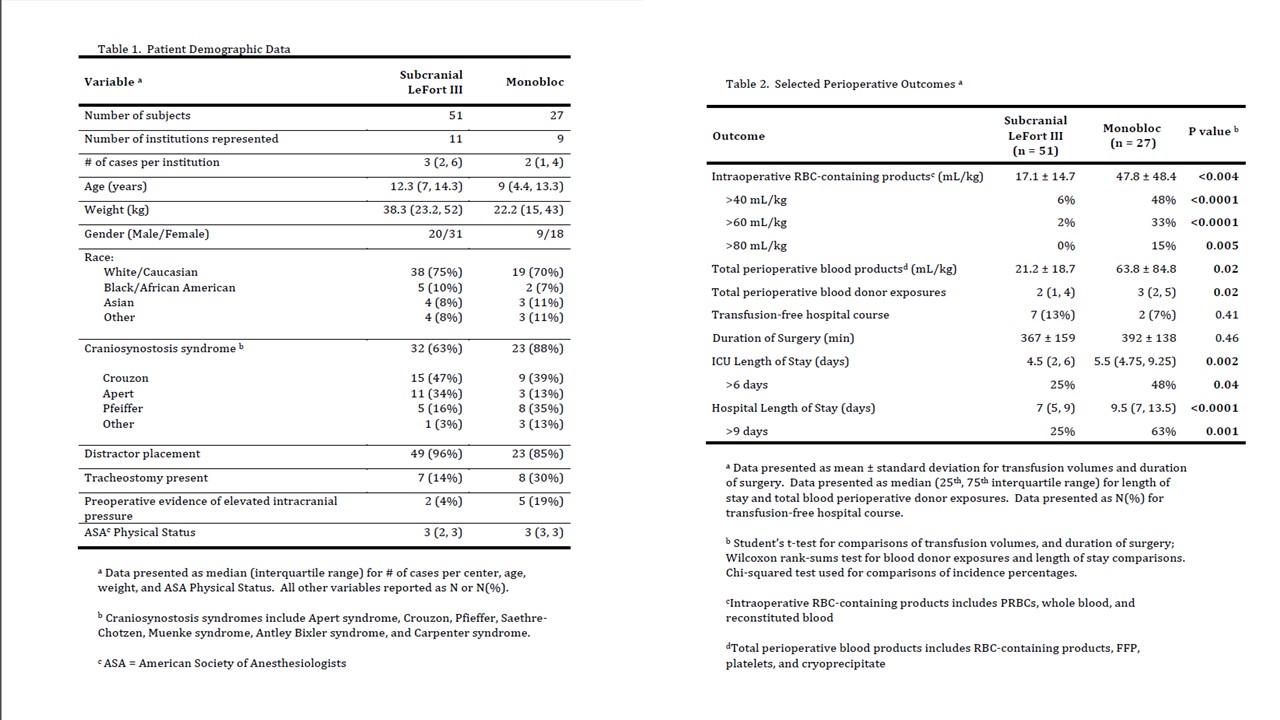
78 total cases were analyzed: 51 children underwent subcranial LeFort III procedures and 27 children underwent Monobloc advancement procedures. The most common diagnosis for undergoing LeFort III or Monobloc was Crouzon’s syndrome. Perioperative management between the 2 procedures showed significance in the following: intraoperative RBC transfusion volume, total blood products, number of perioperative blood donor exposures, ICU length of stay, and hospital length of stay. The percentage of patients staying > 6 days in the ICU and in those staying > 9 days was also significant. Major overall perioperative complications were similar between Lefort III and Monobloc surgeries. Intraoperative complications include hypotension and dural tears and postoperative complications include unplanned secondary surgery, surgical site infections, and respiratory failure.
We present the first comprehensive description of the perioperative management, outcomes, and complications from a large group of North American children undergoing LeFort III and Monobloc midface advancement procedures. This provides evidence this subpopulation in the PCSPR have recovery profiles complicated by blood exposure, prolonged ICU stay, and perioperative complications, moreso in patients undergoing Monobloc surgery than Lefort III osteotomy.
-
 OS2-149 Image 3
OS2-149 Image 3 -
 OS2-149 Image 2
OS2-149 Image 2 -
 OS2-149 Image 1
OS2-149 Image 1
Top










