
NM-314
The effect of transesophageal probe placement on endotracheal tube cuff pressure and perioperative reintubation in congenital cardiac surgery
Pan S, Ingram A, Nguyen K, Blasiole B, Phadke A, Callahan P, Adams P
Children's Hospital of Pittsburgh of UPMC, Pittsburgh, PA, USA
Introduction:
High endotracheal tube (ETT) cuff pressure (CP) during mechanical ventilation is associated with reduced mucosal blood flow and ischemia that can result in perioperative airway complications. Studies in adults have shown that transesophageal echocardiography (TEE) probe placement significantly increases ETT CP. This study aimed to determine if there is a significant increase in ETT CP in children after TEE insertion and whether lower tracheal perfusion pressure during surgery with CPB is associated with postoperative reintubation.
Method:
Patients who underwent cardiac surgery with cardiopulmonary bypass (CPB) and intraoperative TEE were recruited into this prospective observational study. ETT CP was measured following anesthesia induction and endotracheal intubation, after adjustment for CP <25 mmHg prior to TEE insertion, after TEE insertion, after readjustment for CP <25 mmHg (CP CPB), and at the end of the anesthetic (CP final) prior to extubation or transfer to the cardiac intensive care unit. Patients were followed for postoperative reintubation.
Results:
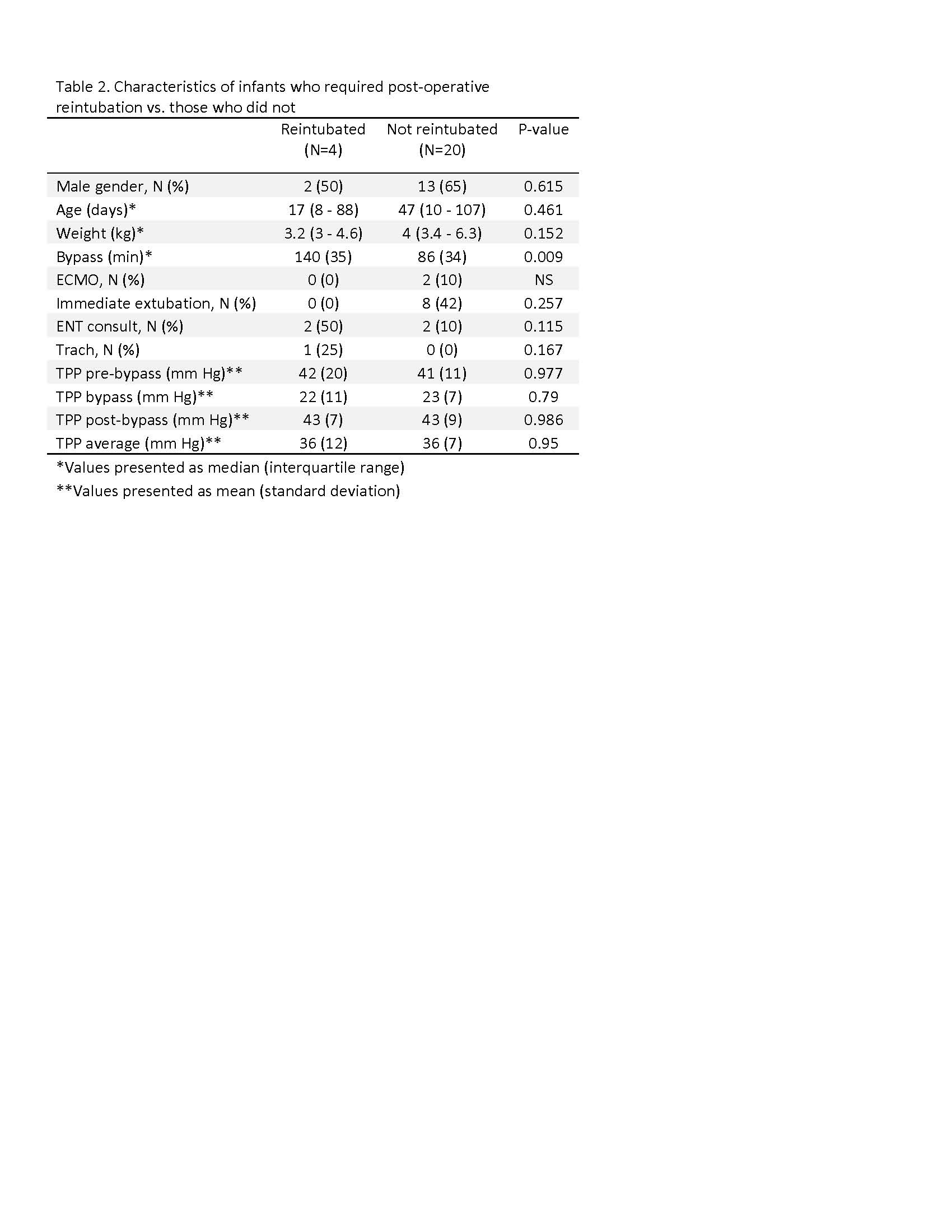
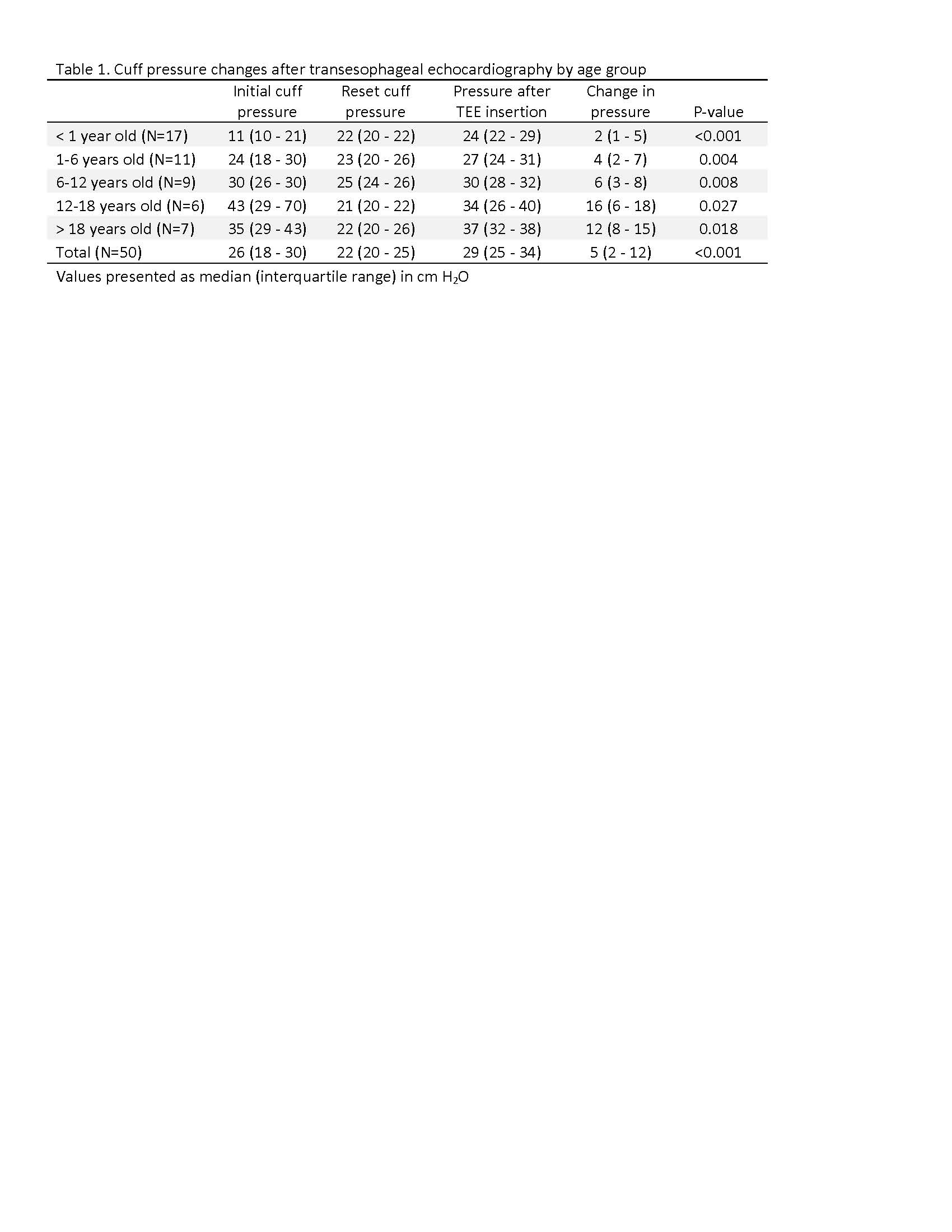
Total of 59 patients (aged 4 days to 42 years old, median 3.9 years old). Nine (15%) patients did not have initial CP data. ETT CP increased significantly after TEE probe insertion in each age group and overall, however the magnitude of change was less for younger patients (Table 1). Four (7%) patients required reintubation and all 4 were infants. Number of reintubations ranged from 1-4 with 1 tracheostomy for the infant reintubated 4 times. Investigation within the infant group showed no significant difference in tracheal perfusion pressure (mean arterial pressure – ETT CP) during the pre-bypass, bypass, post-bypass, or average total anesthesia duration between those who required reintubation and those who did not (Table 2).
Discussion:
We observed an increase in ETT CP with TEE probe placement across age groups and overall consistent with previous adult studies. The magnitude of change in CP may be less in infants and young children because they have more compliant tracheas than adolescents and adults. Interestingly, all reintubations involved infants; however these did not appear to be correlated with ETT CP or tracheal perfusion pressure. This data suggests endotracheal cuff pressure in children may not be the best indicator for perioperative reintubation risk after congenital cardiac surgery with CPB.
Conclusion:
TEE probe placement results in small increases in the ETT CP in children undergoing cardiac surgery. Factors beyond intraoperative ETT CP likely play a role in postoperative reintubation.
-
 NM-314 Image 2
NM-314 Image 2 -
 NM-314 Image 1
NM-314 Image 1
Top










