
AET-25
Do children with Down Syndrome / Trisomy 21 have higher risk of perioperative airway complications?
Soria C, Brzenski A, Graber T
University of California, San Diego, San Diego, California, United states
Introduction
Down Syndrome (DS) features include craniofacial abnormalities, obstructive sleep apnea (OSA), congenital heart disease, atlanto-axial instability, mental retardation, short stature, obesity, and hypotonia. Craniofacial abnormalities include macroglossia, microdontia, mandibular hypoplasia, adenotonsillar hypertrophy, hypotonia, airway malacia, short neck, narrow palate, subglottic stenosis, and choanal atresia. Children with DS may present for multiple surgical procedures such as tonsillectomy and adenoidectomy, myringotomy tubes, and repair of congenital heart defects and gastrointestinal malformations.
Current literature frequently states that DS patients have higher rates of anesthetic complications such as difficult intubation, difficult mask ventilation, bronchospasm, and post-extubation stridor and airway obstruction. However, anecdotally, most pediatric anesthesiologists have not found this to be true. Nevertheless, anesthesiologists are advised to prepare additional rescue airway equipment and consider overnight admission or longer recovery unit stays.
Study Question/Aims/Hypothesis
This study aimed to determine the true incidence of airway complications in DS patients. The hypothesis was that there is a low incidence of airway complications, including difficult intubation, difficult mask ventilation, bronchospasm, and post-extubation stridor and airway obstruction in DS patients.
Methods
This study was a retrospective chart review looking at the pre-anesthetic evaluations, intra-operative anesthetic progress notes, and post-anesthetic operative summaries of patients with DS who underwent anesthesia from the time period of April 1, 2012 to August 31, 2017 at Rady Children’s Hospital in San Diego, California. All patients with a diagnosis of Down Syndrome or Trisomy 21 were included, including all genders, ethnicities, and co-morbidities, from birth to twenty-one years of age. The following patient variables were analyzed: age, height, weight; past medical history; type of surgery; ASA classification; pre-medication; induction method; airway exam; Cormack-Lehane grade; ETT or LMA size; perioperative airway complications (hypoxia, bronchospasm, stridor, difficult intubation or mask ventilation).
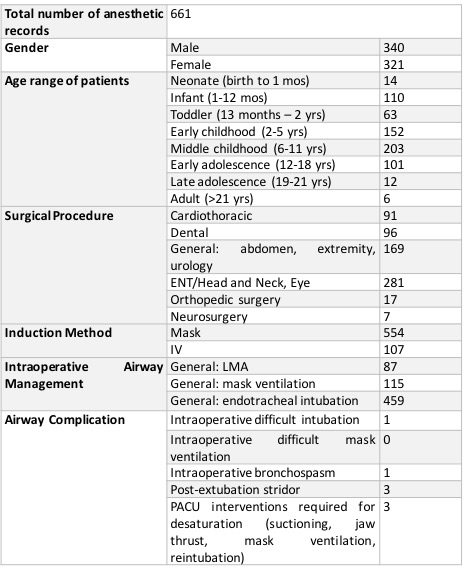
Results
(see Table 1)
Discussion
Our study showed a 1.21% incidence of perioperative airway complications. This supports our hypothesis that Down syndrome is not associated with increased risk of airway complications. Anesthesiologists do not need to take unnecessary precautions that result in overutilization of equipment, staffing, OR and PACU time, and cause scheduling delays and increase medical costs.
-
 AET-25 Image 1
AET-25 Image 1
Top










